Berry, P., Enright, P., Varangu, L., Singh, S., Campagna, C., Gosselin, P., Demers-Bouffard, D.,Thomson, D., Ribesse, J., & Elliott, S. (2022). Adaptation and Health System Resilience. In P. Berry & R. Schnitter (Eds.), Health of Canadians in a Changing Climate: Advancing our Knowledge for Action. Ottawa, ON: Government of Canada.
Lead Author
Peter Berry (Health Canada)
Contributors
Paddy Enright (Health Canada and University of Waterloo)
Linda Varangu (Canadian Coalition for Green Health Care)
Shanaya Singh (Health Canada)
Céline Campagna (Institut national de santé publique du Québec and Centre Terre, Eau, Environnement of the Institut national de la recherche scientifique)
Pierre Gosselin (Institut national de santé publique du Québec and Centre Terre, Eau, Environnement of the Institut national de la recherche scientifique)
David Demers-Bouffard (Institut national de santé publique du Québec)
Changes in climate are affecting the health of Canadians and their health systems. Recent floods, wildfires, extreme heat events, and severe storms have had impacts on health facilities and disrupted care to those in need. Adaptation measures such as assessments of risks and vulnerabilities, integrated surveillance and warning systems, health professional training, and public education can help prepare Canadians and build the climate resilience of health systems. Well-designed efforts to adapt to climate change impacts and reduce greenhouse gas (GHG) emissions within and outside of the health sector can result in very large and near-term co-benefits to health. Many health authorities in Canada are increasing adaptation efforts. However, disparities in efforts exist across the country and adaptation needs to be rapidly scaled up to protect health as Canada continues to warm.
Key Messages
The effects of climate change on health and on health systems in Canada are already evident and will worsen if existing vulnerabilities are not addressed and if gaps in health adaptation are not closed.
Efforts to adapt to climate change — focusing on its health impacts — can significantly reduce current and future impacts on individual Canadians, communities, and health systems.
Climate change impacts on health pose significant economic costs to Canadians, and these costs will increase in the future unless Canada adapts effectively.
Canadian health authorities are undertaking a range of measures to adapt to climate change but are still lagging in many climate change and health actions to respond to the growing risks to Canadians.
Many health authorities are not considering key drivers of vulnerability for specific population groups and therefore may not be addressing important aspects of adaptation for people disproportionately affected, such as First Nations, Inuit, and Métis peoples, racialized populations, seniors, women, and those of lower socio-economic status.
Individual Canadians need to increase preparedness for climate change impacts. Many still need to take necessary measures to protect themselves and their loved ones from growing risks to health.
Health authorities must take measures to increase the climate resilience of health systems. This means ensuring they remain operational when threatened by hazards and sustainable over the longer term, which is one of the most effective ways to protect human health and well-being from the impacts of climate change. Adaptation measures must be scaled up rapidly and substantially if current and future health impacts are to be reduced.
Protecting Canadians from climate change requires a commitment to Indigenous leadership and partnership in research and adaptation efforts, including engaging with Indigenous Peoples in a meaningful way and recognizing and using Indigenous knowledge in a respectful way.
Major co-benefits to human health can be achieved when decision makers in other sectors (such as water, transportation, energy, housing, urban design, agriculture, conservation) promote health and health equity through the design and implementation of actions to adapt to climate change and mitigate GHGs.
Strong measures to reduce GHGs are needed to protect Canadians, their communities, and their health systems from climate change. The health sector can show leadership in reducing its carbon footprint and improving environmental sustainability, while building resilience to future climate change impacts.
WHO, 2022, Working paper on measuring climate resilience of health systems.
10.1
Introduction
Share
Recent scientific research has identified potentially more severe impacts of climate change on societies, including on human health and health systems, at more modest increases in global mean temperatures (Hoegh-Guldberg et al., 2018; Ebi et al., 2019). These findings, along with the goal of “enhancing adaptive capacity, strengthening resilience and reducing vulnerability to climate change” in the Paris Agreement (UNFCCC, 2015, p. 9), have increased recognition among health sector officials of the importance of adaptation measures to prepare for the health impacts of climate change.
Haines and Ebi (2019, p. 271) suggest that, “Climate change is causing injuries, illnesses, and deaths, with the risks projected to increase substantially with additional climate change, threatening the health of many millions of people if there are not rapid increases in investments in adaptation and mitigation.” Growing threats to the health of Canadians from current climate variability and future climate change, as documented in other chapters of this assessment, require health authorities and individual Canadians to proactively prepare for the impacts.
Adaptation measures that get ahead of the curve of increasing climate impacts on ecosystems, infrastructure, communities, and health systems will need to move beyond incremental approaches to adopt transformative changes. Transformational adaptation directly addresses drivers of risks, including underlying vulnerability factors, and contributes to adaptive capacity, and resilience while enhancing social equity and gender empowerment (Crump et al., 2019). The term resilience is used in this chapter to refer to “the capacity of social, economic, and environmental systems to cope with a hazardous event or trend or disturbance, responding or reorganizing in ways that maintain their essential function, identity, and structure, while also maintaining the capacity for adaptation, learning, and transformation” (IPCC, 2014, p. 5). Effective action to protect health also requires health authorities and their partners to rapidly bring proven interventions to scale (Ebi, 2016; Patz & Thomson, 2018).
Previous science assessments increased knowledge of how weather, climate, and the health of Canadians are inter-related; how risks might be expected to increase as the climate continues to rapidly warm and become more variable; and what actions are needed to protect populations. They also highlighted that the resilience of health systems and the willingness of decision makers to take needed adaptive actions will largely determine whether and how much future climate change disrupts communities and affects health and quality of life (Berry, 2008).
Specific findings related to the adaptation process and measures being implemented by individual Canadians and health systems included the following (Berry, 2008; Berry et al., 2014a):
Roles and responsibilities for health adaptation in Canada have been identified in some areas.
Many adaptation actions are being taken by health authorities at all levels of government and by voluntary organizations, including some examples of mainstreaming climate change information into current programs and policies.
There are significant gaps in knowledge of the effectiveness of adaptations.
Gaps in existing adaptation efforts and abilities to cope with risks, combined with widespread exposure to climate-related hazards, indicate significant vulnerability to the health impacts of climate change.
Health systems in Indigenous communities are vulnerable to the impacts of climate change and there are significant challenges in the capacity to adapt and protect health.1
Projected health, demographic, and climate trends suggest vulnerability will continue to increase.
Without ramped-up efforts to adapt, health and social services will come under increasing pressure from climate change impacts, such as extreme weather events and disasters.
There are significant opportunities to adapt, stemming from health officials’ growing interest and awareness of threats from climate change, new tools to develop needed measures, and individual Canadians’ ability to shift their behaviour and architectural practices to adjust to changing climate conditions.
If land-use planning, infrastructure development, emergency preparedness, environmental management, transportation planning, and climate adaptation activities fail to incorporate human health considerations, Canadians will become more vulnerable to climate change impacts on health.
Climate change impacts may exceed the thresholds of current health and related systems (e.g., surge capacity, infrastructure design), which were designed based on assumptions of a stable climate that are now decades old.
The increasing probability of cumulative and/or irreversible impacts means there may be limits to adaptation and the ability to protect individuals and communities from some impacts on health.
Health authorities at all levels of government need to make tailored adaptation efforts due to differences in demographic and health trends, resources and expertise, health care and social service delivery, infrastructure, and community design.
Many health and emergency management authorities must mobilize around and proactively plan for climate change impacts. Leadership and multi-sectoral actions on the issue are needed to make strides in preparing Canadians.
This chapter reviews the development of knowledge since 2012 to build on these findings. It examines current impacts of climate variability and change on health systems in Canada and the state of health adaptation by health authorities and individual Canadians. Opportunities to increase the resilience of individuals, communities, and health systems, as well as challenges to such efforts, are examined to support health officials’ efforts to prepare for future impacts. Analysis draws upon findings and recommendations from previous national assessments and other sources, to explore whether progress is being made in preparing for the impacts of climate change on health in Canada.
10.2
Methods and Approach
Share
A number of research projects were commissioned for development of this chapter, including studies on:
current levels of adaptation by Canadian health authorities;
opportunities and barriers to health adaptation in Quebec; and
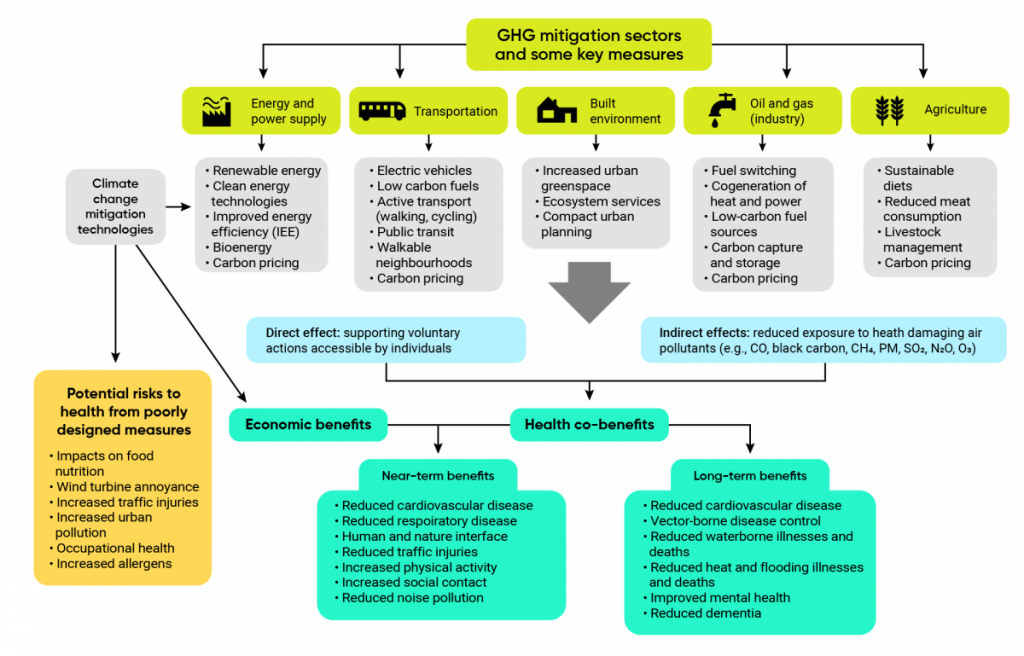
health co-benefits of greenhouse gas (GHG) mitigation measures.
10.2.1
Current Levels of Adaptation by Canadian Health Authorities
Share
An online survey of the status of Canadian health authorities’ actions to prevent, respond to, and adapt to the impacts of climate change and the adaptive capacity and vulnerability of health systems in Canada was conducted in both official languages. The survey examined which climate risks health authorities addressed most frequently, populations considered to be at highest risk, and current adaptation activities. In total, 219 participants representing local to national health authorities across Canada were invited to complete the online survey. Online survey data collection took place from January 17 to March 13, 2019 (eight weeks). A total of 80 surveys were completed with the following breakdown: Atlantic provinces 7; Quebec 11; Ontario 34; Prairie provinces 13; British Columbia and the territories 15.
10.2.2
Opportunities and Barriers to Health Adaptation in Quebec
Share
Given that the province of Quebec has developed the earliest and most extensive climate change and health program in Canada, this study examined the level of adaptation to climate change in the Quebec health sector to understand factors that can influence the integration of the climate change dimension, mainly adaptation, in these organizations. To determine the factors that may have influenced climate change adaptation in Quebec’s health sector, a literature review and interviews with representatives of the health community were conducted. The literature review, conducted in May 2019, identified the factors that facilitate or hinder the implementation of climate change adaptation actions by public institutions, and the results were used as the basis for the interview questions. This was an exploratory review of the literature, since the quality assessment and methodological rigour of the selected studies were not in sufficient depth to qualify as systematic. The EBSCOhost by Web of Science and Google Scholar search engines were used for the research.
Interviews were conducted between July 2019 and November 2019. Participants in the study represented regions across the province and a variety of health-sector functions related to climate change. In total, 49 people were interviewed, including 25 officials from 16 of Quebec’s 18 health regions. The majority of individuals work in environmental health, but others working in occupational health, infectious diseases, health promotion, monitoring, construction, and civil safety were also interviewed. Seven officials from the Institut national de santé publique du Québec (INSPQ) and seven from the Ministère de la Santé et des Services sociaux (MSSS) were also interviewed, as were two people from Ministère de l’Environnement et de la Lutte aux changements climatiques. A total of eight officials from Centres intégrés de santé et des services sociaux (CISSS) and Centres intégrés universitaires de santé et des services sociaux (CIUSSS) also participated in the study.
10.2.3
Health Co-Benefits of Greenhouse Gas Mitigation Measures
Share
This study examined evidence of health co-benefits or risks from GHG mitigation technologies, with a focus on Canada. Background information on the current knowledge of health co-benefits or risks was obtained through a literature review. Articles identified were then reviewed by title and abstract, based on established inclusion criteria. Papers had to discuss known climate change mitigation technologies or policies; how they reduce or mitigate GHGs, short-lived climate pollutants, or air pollution; and at least one corresponding human health co-benefit and/or associated co-risk. Peer-reviewed journal articles, reports, and books were included. Review articles were excluded from the analysis but were used for background information for the literature review. The structured review of literature was done from July to October 2018 and was conducted using the electronic databases EMBASE, MEDLINE, and Global Health.
10.3
Health Adaptation to Protect Canadians
Share
10.3.1
Health Adaptation Actors
Share
Measures to help people prepare for the impacts of climate change can significantly reduce health risks as the climate continues to change (Smith et al., 2014; Campbell-Lendrum et al., 2015; Ebi et al., 2018a; WHO, 2018c; Haines & Ebi, 2019). By and large, the risks to health presented by climate change are not new; public health authorities have years of experience and evidence-based learnings about measures to address the health effects of air and water pollution, contaminated food, vector-borne diseases, ozone depletion, and extreme weather events (e.g., extreme heat events, floods, droughts, wildfires, ice storms, hurricanes) (Frumkin et al., 2008; Séguin, 2008; WHO, 2013; Ebi & del Barrio, 2017).
Preparing for the health impacts of climate change requires a wide range of actors in society to adapt at multiple temporal and geographic scales that take into account complex drivers and feedback mechanisms of the human–environment system (Crump et al., 2019). Adaptation actors include individual Canadians (all Canadians, but particularly people at highest risk of impacts) (see Chapter 9: Climate Change and Health Equity and Chapter 2: Climate Change and Indigenous Peoples’ Health in Canada), health sector decision makers in and outside of government, health care and social services professionals (e.g., doctors, nurses, home care providers, social workers, pharmacists), officials in other health-related sectors (e.g., water systems), and researchers. Health sector adaptation includes health officials, in collaboration with those in other fields, taking action to understand, assess, prepare for, and help prevent the health impacts of climate change, particularly on the highest-risk populations. It includes designing, implementing, monitoring, and evaluating specific measures to reduce health risks (Ebi & Semenza, 2008) and includes broader efforts to increase the climate resilience of health systems. Programs, policies, and measures are most effective in the shorter and longer term if they concomitantly address inequities and boost general population health, which is the foundation of climate-resilient individuals and communities.
10.3.2
Health Adaptation Process
Share
Adaptation planning by health authorities will often focus on efforts to reduce priority risks from specific climate hazards already affecting population health (e.g., development of heat alert and response systems [HARS]), surveillance of emerging or new vector-borne diseases, interventions to reduce health risks of wildfire smoke), or hazards that threaten health in the future. Health adaptation and resilience-building should move society beyond simple coping, which is reactive and concerned primarily with minimizing the immediate damage from a particular climate-related impact. Reactive coping responses often lead to greater vulnerability in the face of increasingly severe climate change threats. By contrast, health adaptation and resilience-building provide a way for health authorities to seize the opportunity climate change presents (Watts et al., 2018) to build more equitable and effective health systems. This may be accomplished, for example, by developing and implementing systems-level changes and by refining targeted actions, such as early warning systems, including HARS. Such actions build social capital and networks (e.g., buddy system to check on neighbours requiring assistance) and remove barriers to treatment and recovery during and after climate events for disadvantaged populations.
Health adaptation is most effective when it is anticipatory and proactive given that the climate continues to change in Canada at an increasing rate creating greater risks to health, some of which may surprise, disrupt, and challenge health authority activities. It is also evidence-informed and future-facing, to include measures that protect populations from more severe projected health risks, which may occur earlier than expected. Iterative processes for adaptation risk management (e.g., regular climate change and health vulnerability and adaptation assessments, evaluation of adaptation effectiveness, Indigenous partnerships, stakeholder engagement) help to ensure that adaptation actions address uncertainty of timing, severity, and geographical extent of future climate change impacts, including the potential for non-linear risks to health (Ebi et al., 2016a; Hess & Ebi, 2016; Ebi & del Barrio, 2017). Non-linear risks to health arise from much more severe climate impacts that are low probability but potentially high consequence events. The extreme heat event that affected northwestern United States and British Columbia in July 2021 and that is likely to have contributed to over 700 deaths in that province (Roffel, 2021) was estimated to be a 1 in 1000 year event (Philip et al., 2021).
Knowledge of how health authorities undertake adaptation has increased (Lesnikowski, 2011; Paterson et al., 2012; Ebi & del Barrio, 2017). Effective health adaptation plans and measures are grounded in the following considerations:
The adaptation process is instigated and energized by increased awareness and knowledge of climate change risks to health in a jurisdiction (Lesnikowski, 2011; Eyzaguirre & Warren, 2014).
National and international health authorities and research institutions identify climate change as a priority and provide adequate funding to enable understanding of complex drivers of health outcomes across environmental, social, and human systems (Ebi et al., 2016b).
Groundwork activities (e.g., capacity building, monitoring and surveillance, research) often precede and support concrete adaptation actions (e.g., information-sharing, infrastructure development, technology and innovation, management and planning, policy development, resource transfers and funding support) (Lesnikowski, 2011; Shah et al., 2018).
Health adaptation measures are informed by scientific and/or Indigenous knowledge2 gained through a climate change and health vulnerability and adaptation assessment or other knowledge-development activities (Shin & Ha, 2012; WHO, 2013; Berry et al., 2018; Watts et al., 2018).
Health adaptation activities are developed and implemented with knowledge and consideration of linkages to complementary GHG mitigation measures (ACT, 2018), as there are significant opportunities to increase health co-benefits of actions and to reduce possible health risks (Haines et al., 2009; Martinez et al., 2018; Haines & Ebi, 2019).
Adaptations to protect health are mainstreamed into existing policies, plans, programs, and budgets and are iterative and subject to regular monitoring for effectiveness and enhancement opportunities through adaptive management (Ebi, 2011a; WHO, 2013; Wheeler & Watts, 2018). The climate and other important drivers of health outcomes (e.g., health systems, demographics) will continue to change, resulting in uncertain futures (Sellers & Ebi, 2017).
Health adaptation actions are most effective when they are undertaken to advance health system resilience and root causes of vulnerability, and when they consider maximizing public health and health equity co-benefits. They are identified through community consultations with a range of partners that are either highly exposed to climate hazards and/or may lack capacity to adapt. These populations can include First Nations, Inuit, and Métis peoples, women, people living with disability, seniors, immigrants, low-income residents, minority language communities, outdoor workers, people exposed to environmental pollution, people with preexisting illnesses, people without access to insurance, public housing residents, refugees, lone-parent households, students, those experiencing homelessness, and young children (Gould & Rudolph, 2015; Deas et al., 2017; Dodd et al., 2018; NASEM, 2018).
Adaptations to protect health are intentionally and specifically focused on climate change impacts (Dupuis & Biesbroek, 2013) and strive to reduce risks from current climate hazards as well as future more severe and frequent impacts, including the possibility of compounding and cascading events (Sellers & Ebi, 2017; Glasser, 2019).
Health authorities take a broad health systems approach to adaptation, to identify and address vulnerabilities existing in any and all components of health systems to make them climate-resilient to withstand possible impacts on health facilities (WHO, 2015; Balbus et al., 2016; Ebi et al., 2018b).
Collaboration among a multitude of sectors that support and maintain the determinants of health (e.g., social housing, water systems managers) is required to prepare successfully for climate change impacts on health.
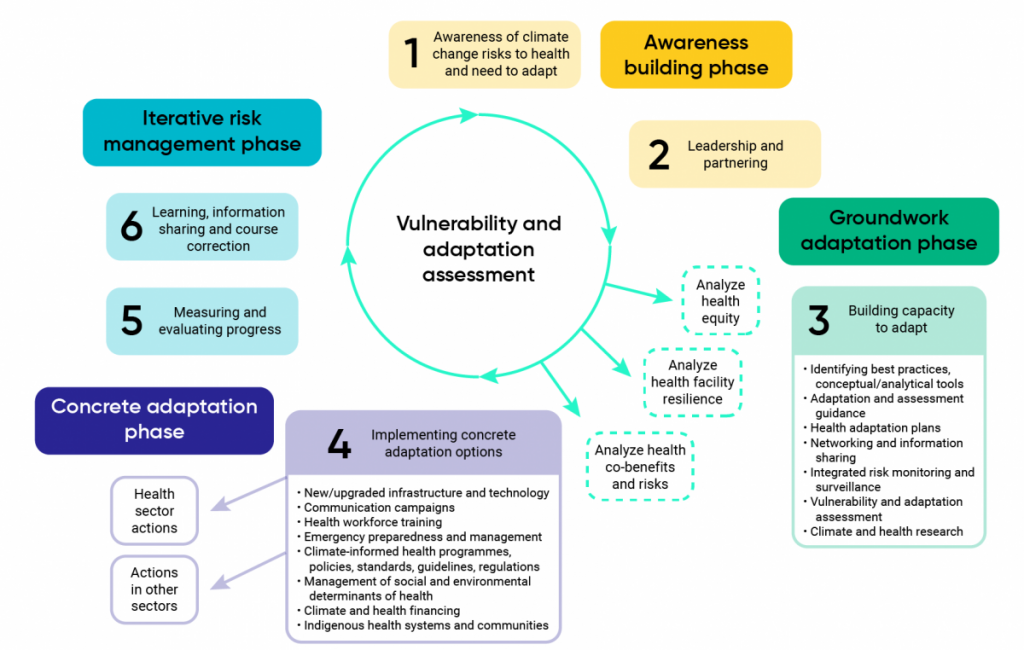
Figure 10.1 presents a framework that highlights the stages health decision makers go through when adapting to climate change risks, informed and initiated by a vulnerability and adaptation assessment for climate change and health. Table 10.1 proposes indicators of climate-resilient health system adaptation for Canada based on this framework.
Uptake of climate change and health communication campaigns (e.g., page or video views, observable changes in behaviour, etc.)
Climate change and health information on health authority websites (e.g., climate change impacts to health and suggestions for behavioural changes that may reduce negative health outcomes)
Number of climate change and health research projects completed relative to peer jurisdictions with results disseminated
Media coverage of climate change and health issues
Social media engagement on climate change and health issues
Groundwork adaptation phase
Leadership and partnering
Proportion of jurisdictions (e.g., communities, provinces, territories and/or regions) with climate change action plans that include measures to protect health
Proportion of jurisdictions (e.g., communities, provinces, territories and/or regions with climate change and health offices/focal points)
Number of key stakeholders (e.g., water authorities, community housing groups, assisted-living facilities, school boards, etc.) including climate change and health information in risk assessments
Vulnerability and adaptation assessment
Proportion of local to national health authorities that have completed climate change and health vulnerability and adaptation assessments
Proportion of local to national adaptation and mitigation policies with health impact assessments
Integrated risk monitoring and surveillance
Proportion of local to national health authorities with integrated early detection tools and surveillance systems to identify changing health risks and impacts (for example, see Chapter 6: Infectious Diseases)
Proportion of local to national health authorities with established climate-informed early warning systems for extreme whether events and disease outbreaks (e.g., droughts, floods, zoonotic and vector-borne diseases)
Climate and health research
Coordinated national research agenda on climate change and health
Number of climate change and health research programs and networks
Number of academic publications on climate change and health relative to peer jurisdictions
Completion of health research sex- and gender-based analysis training
Concrete adaptation phase
Health workforce training and education
Proportion of health professional education and training programs (e.g., medical school, nursing, and public health programs) with course offerings on climate change and health
Proportion of health professionals (e.g., doctors, nurses, pharmacists, public health officials) who have received climate change and health training
New/upgraded infrastructure and technology
Proportion of health facilities with contingency plans (e.g., surge capacity) for the deployment of sufficient health personnel in case of acute shocks
Proportion of health facilities that have reported the completion of a climate-resilience assessment
Proportion of health facilities with climate-resilience informed programming
Proportion of health facilities that report adaptation of new technologies and products to improve resilience
Indigenous health systems and communities
Surveillance and early warning capacity for Indigenous communities
Availability of comprehensive, reliable, and culturally specific climate change and health indicators
Access to diagnosis and treatment for physical and mental health conditions, including climate-sensitive diseases
Established climate change and health focal point in regional to national health authorities
Community knowledge and awareness of climate change imopacts on health
Public health work force available and trained in culturally appropriate climate change research, surveillance, and adaptation
Status of water and food security and sovereignty
Resilience of health care facilities in Indigenous communities
Climate and health funding
Local to national funding for climate change and health research by issue, region, and population (e.g., Indigenous populations, seniors, children, immigrants)
Local to national funding for climate change and health action plans, strategies, and adaptation measures
Local to national funding for climate change and health organization capacity (e.g., office/focal point for climate change and health)
Climate-informed health programs, policies, standards, guidelines, regulations
Proportion of health authorities with public health programs addressing key climate risks and hazards using most recent climate projection information
Proportion of health authorities with public health programs addressing at-risk populations (e.g., children, seniors, immigrants) using the most recent climate projection information
Proportion of sectors important to health (e.g., industry, energy, agriculture, housing, urban design, water, transportation) integrating climate change and health information into adaptation and GHG mitigation plans, strategies, and measures
Emergency preparedness and management
Proportion of local to national public health and health care authorities and facilities with emergency plans that address climate-related hazards and growing risks
Proportion of local to national strategies for disaster risk reduction that include consideration of risks to health from climate-related hazards
Management of social and environmental determinants of health
Robust local to national plans to reduce GHGs to meet agreed-upon international targets
Established integrated monitoring systems for analysis of environmental hazards and health risks from climate change
Existence and enforcement of regulatory standards on air quality, water quality, chemical discharges, and waste disposal and management
Food security rates among climate-sensitive populations
Access to services that support environmental and social determinants of health (e.g., access to safe water, adequate housing, employment, energy, and food security) among Indigenous populations
Identifying best practices, conceptual/analytical tools
Number of tools developed and implemented to support health adaptation actions
Adaptation and assessment guidance
Climate change and health vulnerability and adaptation assessment guidance developed and disseminated for use by health authorities
Health adaptation plans
Number of climate change and health adaptation plans or strategies developed
Networking and information-sharing
Number of climate change and health networking and information-sharing mechanisms (e.g., communities of practice) being used to support health adaptation
Iterative risk management phase
Measuring and evaluating progress
Proportion of completed local to national climate change and health vulnerability and adaptation assessments that have a monitoring and evaluation plan
Proportion of local to national health authorities that have completed more than one climate change and health vulnerability and adaptation assessment under an ongoing schedule
Number of local to national health authorities that include climate change and health indicators in regular health reports to the public
Learning, information-sharing, and course correction
Existence of and participation in local to national initiatives for information and knowledge-building on climate change and health (e.g., communities of practice)
Source: Lesnikowski, 2011; Watts et al., 2015; WHO, 2015; Elliot et al., 2017
10.3.3
Health Adaptation Challenges and Opportunities
Share
Health decision makers can find adapting to climate change challenging if they do not have the required technologies (e.g., new vaccines, communications, data sharing), information and skills (e.g., projections of health risks, training of health authorities), infrastructure (e.g., climate-resilient health facilities), resources, and institutional arrangements (e.g., a climate change and health focal point) (Frumkin, 2011). Barriers can also include a lack of authority and leadership for action, a narrow framing for public health interventions that omits action on root causes of vulnerability, legal obstacles, and failures in collective decision making (Ford & King, 2015; Gould & Rudolph, 2015). Some health systems in rural, remote, and/or Indigenous communities are already affected by existing vulnerabilities that increase risks from climate change impacts, for example, higher rates of all-cause mortality, less surge capacity during emergencies, reduced access to health facilities, and difficulty in retaining health professionals and accessing specialized health care (DesMeules & Pong, 2006; Vodden & Cunsolo, 2021) (see Chapter 2: Climate Change and Indigenous Peoples’ Health in Canada). Health systems and communities with fewer resources have greater difficulties responding to impacts and recovering in ways that protect the health of populations. In Canada, federal and provincial/territorial levels of government have a key role to play in supporting preparedness activities for local health authorities by building capacity through information-sharing, coordination, developing and disseminating scientific information, and financial contributions (Austin et al., 2019). Adaptation to the effects of climate change will be much greater and ability to protect health will be much more limited without strong measures to reduce GHGs (IPCC, 2014; Wheeler & Watts, 2018).
No population group or Canadian region should bear an unreasonable portion of the costs associated with the health and social impacts of climate change. Existing social inequities within a community (e.g., income, water insecurity, food insecurity, chronic health disparities) and/or higher rates of disease burdens can reduce the adaptive capacity of specific subpopulations (UNEP, 2018; Friel, 2019). Populations and communities that lack the capacity to plan for, respond to, and recover from climate change impacts will remain disproportionately affected by climate hazards (Berry et al., 2014a; Crump et al., 2019). In Canada, this may include rural and remote communities, Indigenous Peoples and communities, racialized populations, low-income populations, people with mobility challenges, people who are socially isolated, immigrants, renters, outdoor workers, minority language communities, seniors, and people with chronic diseases. In some cases, individuals may be subject to multiple, possibly intersecting, vulnerability factors. For instance, rural and remote residents, in addition to being more geographically exposed to some climatic hazards (e.g., wildfires), are more likely to be elderly, to work outdoors, to have lower average incomes, to have less internet access, and to have higher rates of chronic health conditions. Policies and programs to address existing social inequities and the root causes of vulnerability are needed to plan for climate change impacts on health (CICC, 2021) (see Chapter 2: Climate Change and Indigenous Peoples’ Health in Canada and Chapter 9: Climate Change and Health Equity).
Other challenges to adaptation can arise when efforts to address climate change impacts by decision makers, in or outside of the health sector, are not coordinated and well planned, leading to maladaptation — unintentionally increasing risks to other sectors, social groups, or systems (Austin et al., 2016) (Table 10.2). Insufficient information and/or limited awareness of risk trade-offs can also lead to maladaptation or to insufficient adaptation among individuals to protect themselves and/or their families from the health effects of multiple climate hazards. For example, exercising during cooler parts of the day (e.g., night) or staying in shady areas to reduce risks from heat may lead to greater exposure to mosquitos and ticks that carry vector-borne diseases (Hill, 2012). Actions to plant vegetation like trees on the south side of a home to cool the building may be maladaptive if the trees produce pollen and are located near the intake of the furnace or air conditioner. They may also be maladaptive if vegetation, including leaves and fallen branches, is not maintained and serves to increase the presence of combustible materials near a home or structure that connects to a home, such as a fence. In some contexts vegetation may also harbour disease vectors. Efforts to conserve energy by opening blinds to take advantage of natural light whenever possible may increase risks of heat illness. As well, the use of cooling facilities (e.g., community centres, pools, libraries, malls) and public spaces during extreme heat events to protect health may increase risks from COVID-19 if necessary physical distancing, hand hygiene, and related measures are not taken (Shumake-Guillemot et al., 2020).
Maladaptation to climate change increases the risk that health decision makers will become trapped in a cycle of responding to and treating ever-increasing negative health outcomes in the population. Poorly designed or maladaptive measures may also exacerbate existing inequities, for example, if public information campaigns and funding are lacking (Paavola, 2017). Table 10.2 provides examples of maladaptive actions that can affect health.
Table 10.2
Potential maladaptive actions in efforts to protect health from climate change impacts
Broad type of maladaptive action
Possible health sector examples
Failure to anticipate future climates
Health-related infrastructure (e.g., hospitals, drinking water systems) built or renovated without resilience to future climates
Adaptation actions not taking wider impacts into account
Pollen-producing trees to reduce the urban heat island in urban areas
GHG and air pollutant emission reductions that lead to minimal air quality benefits for disadvantaged neighbourhoods
Engineered defences that preclude alternative approaches and are designed without a health equity lens
Adaptation of infrastructure in other sectors that do not maximize health co-benefits in short or longer term
Awaiting more information, or not doing so, and eventually acting either too early or too late
Awaiting better projections and health data to complete or use results from a climate change and health assessment, thereby forgoing the opportunity for proactive adaptation
Forgoing longer-term benefits in favour of immediate adaptive actions
Focus on treating health outcomes and insufficient efforts to build healthy and climate-resilient communities (e.g., greening to reduce urban heat island effect)
Moral hazard
Encouraging risk taking (e.g., lack of insurance, social safety net, aid backup) such as moving to flood plain or urban/forest interface prone to wildfires
Adopting actions that ignore local relationships, traditions, Indigenous knowledge, or property rights, leading to eventual failure
Development of health adaptation plans without broad consultations and engagement with diverse and representative populations, leading to actions that do not respect unique cultural needs and values (e.g., interventions imposed on Indigenous communities)
Adopting actions that favour one group over others, directly or indirectly, leading to breakdown and possible conflict
Implementation of health adaptations that are not accessible to low-income individuals or those experiencing homelessness (e.g., no heatwave cooling centres in low-income neighbourhoods, social services not accessible by public transit)
Retaining traditional responses that are no longer appropriate
Failure to expand monitoring and surveillance systems to detect new, emerging, or exotic risks to health
Source: Adapted from Noble et al., 2014
There are opportunities for robust adaptation through collaboration among officials in a range of sectors (e.g., health, water, agriculture, energy, housing, environment, conservation, planning, transport, disaster management, and infrastructure) on monitoring and surveillance of climate change impacts on health; identifying higher-risk populations; addressing barriers that limit preparedness (e.g., poverty, inadequate housing and infrastructure, ineffective communications); reducing uncertainty through increased research on impacts; educating the public and decision makers about potential impacts and the benefits of preparedness; and funding needed actions (Séguin, 2008; WHO, 2010; Ebi, 2011b; Frumkin, 2011; Ebi & del Barrio, 2017). For example, technical and operational synergies can be achieved when health authorities and disaster management officials collaborate to improve disaster preparedness and response, communicate risks to the public, and undertake risk and vulnerability assessments and health system resilience-building (Banwell et al., 2018). The Emergency Management Framework for Canada recognizes the linkages between climate change and emergency management and the benefits of multisectoral approaches to resilience-building (PSC, 2017). At the individual level, preparing for climate hazards and taking action to avert impending threats requires information about risks and effective personal protective measures, resources to take action, and a supportive social network, particularly for people who require assistance.
Given increasing risks and potentially severe impacts on health, adaptation activities need to be rapidly scaled up outside of normal health ministry activities (Ebi, 2016). Box 10.1 provides an example of collaboration on adaptation among public health and infrastructure decision makers to reduce risks from climate change affecting children. A major benefit of collaboration among sectors on the design, implementation, and monitoring of adaptation and of GHG mitigation measures is that co-benefits to health from such actions can be maximized (e.g., improved mental health from increased social capital, reduced obesity from active infrastructure), while potential risks to health of the measures can be reduced (Cheng & Berry, 2013; WHO, 2018c) (see section 10.6 Health Co-benefit of Adaptation and GHG Mitigation Measures).
Partnerships with Indigenous Peoples and use of Indigenous knowledge, local context, and values — and incorporating sex, gender, and equity considerations into decision-making — support more effective measures through a respectful and meaningful adaptation process. Such collaboration can increase the relevance of the resulting measures, build capacity, and strengthen resilience through more inclusive and dynamic climate change networks within communities. Community-based adaptation research in Indigenous communities can be conducted through team-building approaches that identify common goals, support the meaningful engagement of knowledge users, and continuously monitor and evaluate progress (Ford et al., 2018) (see Chapter 2: Climate Change and Indigenous Peoples’ Health in Canada).
In recent years, the understanding of adaptation options that modify public health interventions for existing climate-related health hazards or address new and emerging risks, thereby building resilience to climate change impacts on health, has increased (Paterson et al., 2012; WHO, 2015; UNEP, 2018; ISC, 2019). Each chapter of this assessment provides information about adaptation measures to address specific climate change health concerns facing Canadians. Several tools to assess adaptation can be used to examine options for reducing risks, such as forecasting by analogy, screening, multi-criteria decision analysis, comparative risk assessment, benefit–cost analysis, cost-effective analysis, and implementation analysis (WHO, 2013). However, using such tools and prioritizing measures to reduce health risks from climate change can be difficult if there is insufficient information about current and/or projected impacts on health and of the possibility of surprise or unanticipated impacts (Wardekker et al., 2012).
10.3.4
Effectiveness of Health Adaptation
Share
Over the last several decades, the success of public health measures in reducing the health impacts of environmental hazards suggests that adaptations to address climate-related health risks can be effective in protecting populations. Adaptation can delay the increase in health risks from climate hazards at higher levels of warming (CCA, 2019; Ebi et al., 2021). Greater actions to prepare populations and health systems for climate change, and to reduce GHGs, would reduce the future burden of disease (Haines & Ebi, 2019). However, there is a paucity of information on the effectiveness of specific health adaptation measures in and outside of Canada, presenting a significant challenge to decision makers (Bouzid et al., 2013; Anderson et al., 2017). One study that reviewed the effectiveness of 56 specific interventions spanning 14 health issues of concern related to climate change revealed wide divergence among adaptations in terms of evidence (Anderson et al., 2017). Box 10.2 describes how the Texas Medical Centre undertook effective measures to increase its resilience to severe storms.
More investigation has been conducted on the effectiveness of measures to reduce health risks from extreme heat than on health risks from other climate hazards. The scope of discussion in this chapter does not permit review of the effectiveness of all health adaptation measures. Information on the current state of knowledge on the effectiveness of measures to reduce heat-health risks is presented to highlight the importance of regularly evaluating actions to protect health and of integrating uncertainty into the decision-making process.
Several studies suggest that, even with a warming climate, population susceptibility to extreme heat events has not been increasing, or has even been decreasing, in a number of countries (Fouillet et al., 2008; Kyselý & Plavcová, 2012; Schifano et al., 2012; Heudorf & Schade, 2014; Hondula et al., 2015; Arbuthnott et al., 2016; Barreca et al., 2016; Sheridan & Dixon, 2016). Research in regionally and economically diverse countries also indicates that HARS, components of which can include heat-health warning systems (McGregor et al., 2015) and heatwave action plans (HAPs) (Casanueva, et.al., 2019; Jay et al., 2021) can reduce poor health outcomes associated with extreme heat events (Hess & Ebi, 2016; Anderson et al., 2017; Lee, et al., 2019). In 2017, an estimated 47 countries had national or subnational HAPs in place (GHHIN, 2018), including Canada, which has HAPs in many communities and regions.
Sheridan and Allen (2018) suggest that implementation of HARS, greater awareness of heat-health risks, and improved quality of life have helped reduce the health impacts of heat in the developed world. These systems have been shown to be protective in Europe (Matthies et al., 2008; Martinez et al., 2019), France (Fouillet et al., 2008), Italy (Michelozzi et al., 2006; Baccini et al., 2011; Morabito et al., 2012), India (Das & Smith, 2012; Hess et al., 2018), Shanghai (Tan et al., 2007), Hong Kong (Chau et la., 2009), and Milwaukee (Weisskopf et al., 2002). It was estimated that implementing a heat action plan in Ahmedabad, India, in 2010 avoided an estimated 1190 average annualized deaths in 2014–2015 (Hess et al., 2018). However, some studies argue that robust evidence showing that such systems have a discernable influence on health outcomes is lacking (Boeckmann & Rohn, 2014; de’ Donato et al., 2015; Hondula et al., 2015; Weinberger et al., 2018). Well-designed HARS can result in significant economic savings when the costs of systems are compared with their economic benefits. For example, Hunt et al. (2017) calculated the benefit-to-cost ratios of alert systems to be 913 for Madrid, 308 for Prague, and 11 for London.
Many existing health sector policies, programs, and measures aimed at protecting people from extreme heat and other climate hazards and health outcomes (e.g., air pollution, infectious diseases, water-borne diseases, food-borne diseases, extreme weather events) were not designed incorporating information about increasing risks from climate change and so will have limited effectiveness in the future, unless they are modified (Haines & Ebi, 2019). In fact, many HARS are not designed to address increased risks posed by a changing climate, such as alterations in the onset, duration, and intensity of extreme temperatures and resulting health outcomes (Lee et al., 2019). HARS need to be regularly reviewed and evaluated through an iterative process to ensure they are fully protective under new climate conditions and hazards (Health Canada, 2012; Hess & Ebi, 2016; Lee et al., 2019).
In Canada, researchers in Quebec reported that heat alert systems can be effective (Poitras, 2018) and that local and provincial HAPs reduced mortality associated with a severe heat event in 2010 (Bustinza et al., 2013) and in 2018 (Lebel et al., 2019). Benmarhnia et al. (2016) reported that improvements to the Montréal HAP have decreased the number of daily deaths five-fold (see Chapter 3: Natural Hazards). In addition, efforts to warn the public about hazardous heat conditions and poor air quality have been found to be effective in getting people to take protective measures and in reducing costs to the health system (Gosselin et al., 2018; Mehiriz et al., 2018; Mehiriz & Gosselin, 2019). Health authorities in Toronto and Montréal reported that alert systems led to an increased awareness of risks to health from heat and to the uptake of health protective behaviours, such as drinking water, checking for alerts, wearing looser clothing, and seeking cooler locations (Health Canada, 2012; City of Toronto, 2019).
Additionally, preventive adaptation measures to reduce urban heat islands in Quebec (e.g., reduction of concrete/asphalt surfaces, increasing vegetation) were found to be effective in cooling communities and reducing health risks (Beaudoin & Gosselin, 2016; Health Canada, 2020d). From an economic perspective, the benefits of actions to reduce risks to health from extreme heat can justify implementation (Hunt et al., 2017) and may reap large cost savings. Tröltzsch et al. (2012) estimated that, between 2071 and 2100, implementation of a heat alert system in Germany would result in a value of EUR 2.36 billion in avoided deaths and EUR 165 million in hospital savings annually.
More research is required to better understand the effectiveness of adaptations to extreme heat events and to other climate hazards projected to increase in the future (Bouzid et al., 2013; Berry et al., 2014a). National estimates of heat-related morbidity and mortality would benefit from greater standardization of surveillance definitions and practices to enable comparisons among provinces. This evidence base would benefit the design, evaluation, and reporting of future climate change and health adaptation interventions (Hess & Ebi, 2016). For example, Valois et al. (2017) developed a behavioural index composed of 12 adaptations to gauge whether individuals in urban areas are adapting well to high summer temperatures. Studies of effectiveness are important because current health adaptations may not reflect important changes in exposure due to climate change, such as the longer heat season in many regions (Ebi et al., 2016c), including Canada (Zhang et al., 2019).
10.3.5
Status of Health Adaptation
Share
At the global level, some adaptation progress has been made; for example, at least 92 countries have completed vulnerability and adaptation assessments for climate change and health (Berry et al., 2018). However, a health adaptation gap exists that increases the vulnerability of people to climate change impacts (Watts et al., 2015; Martinez et al., 2018; Watts et al., 2018). The World Health Organization (WHO) collects global data every two years on a number of indicators to gauge progress toward preparing for climate change impacts on health. The data are reported through the WHO/United Nations Framework Convention on Climate Change (UNFCCC) Climate and Health Country Profiles (WHO, 2018a). The most recent survey, undertaken in 2017/2018, indicated that there has been progress on climate change and health adaptation internationally, but that adaptation plans and strategies vary widely in terms of their scope and that implementation of specific actions remains a key challenge (WHO, 2019). In addition, the results of vulnerability and adaptation assessments for climate change and health are influencing policy decisions in health ministries in various countries, and many health authorities are increasing collaboration with decision makers on adaptation in other sectors (WHO, 2019).
Analysis of Canada’s progress in addressing climate change risks to health, based on the WHO indicators, suggests that further actions are needed in some areas (Table 10.3).
Table 10.3
Canadian performance on WHO climate change and health resilience indicators
A national focal point for climate change has been identified in the Ministry of Health
Yes
The Climate Change and Innovation Bureau at Health Canada is the national focal point for climate change and health issues (Government of Canada, 2019).
Projects or programs on health adaptation to climate change have been implemented
Yes
Though gaps remain, Health Canada, the Public Health Agency of Canada, the Canadian Institutes for Health Research, and Indigenous Services Canada are undertaking a range of measures to reduce risks to Canadians from climate change associated with extreme heat events, air pollution, and infectious diseases, and to address special challenges faced by Indigenous Peoples living in Northern and Southern communities (Government of Canada, 2019; Government of Canada, 2020a).
Numerous provinces and territories are undertaking climate change and health programming within their jurisdictions.
A national assessment of climate change impacts, vulnerability, and adaptation for health has been conducted
Yes
Séguin, 2008; Berry et al., 2014a
Climate information has been included in the Integrated Disease Surveillance and Response System, including development of early warning and response systems for climate-sensitive health risks
Partially
Early warning systems for climate change health risks are generally the mandate of provincial/territorial and local health authorities. A number of health authorities have developed warning systems for extreme heat events, floods, and air pollution, including real-time surveillance systems that use data on multiple vulnerability factors. Understanding of climate-driven changes affecting infectious disease distribution in Canada are still emerging. However, a number of infectious diseases known to be climate-sensitive (e.g., Lyme disease) are tracked at the national level.
Estimated costs to implement health resilience to climate change have been included in planned allocations from domestic funds in the last financial biennium
Partially
In Canada, health is primarily the responsibility of provinces/territories. Many provinces and territories have begun work to build climate resilience, including through the allocation of financial resources.
Federally, through Budget 2016 and Budget 2017, the Government of Canada committed $125 million over 11 years to help protect the health of Canadians from the impacts of climate change and to increase the resilience of our health systems. These investments support needed activities such as research, education and capacity building. Budget 2021 allocated $22.7 million to support First Nations and Inuit communities in responding to the health impacts of climate change.
National Communication submitted to UNFCCC has included health implications of climate change mitigation policies
Partially
Canada’s seventh National Communication (2017) recognizes the economic and social consequences (including on health) of measures to address climate change but does not provide detailed information or analysis in this regard (Government of Canada, 2017).
Activities to increase climate resilience of health infrastructure have been implemented
Partially
Some health authorities have begun investigating or requiring the assessment of the climate resilience of health infrastructure (BC Health Authorities, 2020; Lower Mainland Facilities Management, 2020).
A National Health Adaptation Strategy has been approved by the relevant government entity
Partially
Canada’s Pan-Canadian Framework on Clean Growth and Climate Change includes a range of actions to address health risks from climate change (Government of Canada, 2015).
The Government of Canada has committed to developing a National Adaptation Strategy (Government of Canada, 2020b).
Actions to build institutional and technical capacities to work on climate change and health have been implemented
Yes
The HealthADAPT program (2019–2022) is building the capacity of 10 health authorities in regions across Canada to increase knowledge of climate change impacts on populations and develop needed adaptation actions (Health Canada, 2019).
The national strategy for climate change mitigation has included consideration of the health implications (risks or co-benefits) of climate change mitigation actions
Partially
The Government of Canada has recognized the need to achieve health co-benefits in the implementation of GHG mitigation measures (Government of Canada, 2020b).
A valuation of co-benefits of health implications of climate mitigation policies has been conducted
Partially
The Government of Canada develops Regulatory Impact Analysis Statements for each proposed GHG regulation that provides information on its objectives and its expected costs and benefits (Government of Canada, 2021). Not all proposed, or implemented, GHG-reduction measures include analysis of health risks or co-benefits.
Estimated costs to implement health resilience to climate change have been included in planned allocations from international funds in the last financial biennium
Not applicable
Canada does not receive funds from international sources to implement actions to protect health from climate change.
Similarly, the Lancet Countdown on Health and Climate Change regularly tracks 41 indicators in five areas to gauge efforts to address climate change impacts on health globally. They include (1) climate change impacts, exposures, and vulnerability; (2) adaptation, planning, and resilience for health; (3) mitigation actions and health co-benefits; (4) finance and economics; and (5) public and political engagement (Watts et al., 2018). Following the methods and indicators of the Lancet Countdown, major medical organizations in Canada, including the Canadian Medical Association, Canadian Public Health Association, and the Canadian Association of Physicians for the Environment began in 2017 to report annually on actions undertaken in Canada (Howard et al., 2017; Howard et al., 2018). To improve Canada’s ability to tackle climate change specific to the health sector, recommendations include support for tele-commuting and telehealth options; creating curricula for all medical and health science faculties related to climate change; communicating the links between climate change and human health to the public; funding research on mental health impacts of climate change; and enhancing efforts to protect Canadians from extreme heat (Howard et al., 2017; Howard et al., 2018).
Two stakeholder workshops were hosted by Health Canada, including one in 2018 to discuss development of a pan-Canadian climate change and health surveillance system, and another in 2016, that brought together provincial and territorial health and environment officials, municipal health units, researchers, non-governmental organizations, and Indigenous partners from across Canada, to explore priority health issues, research gaps, and adaptation needs to prepare Canadians and health systems for climate change. Recommendations and needed actions from the meetings are presented below (Brettle et al., 2016; Knowledge Management, 2018).
Knowledge and data
Develop a pan-Canadian monitoring and surveillance system that is specific for climate change health outcomes and serves the needs of health authorities.
Key climate change and health indicators adopted across Canada and at specific locations that are consistent and standardized with procedures to identify data quality issues.
Increased data on indicators of climate change and health vulnerability, resilience benchmarks, and support for understanding regional vulnerabilities and risk.
Climate change and health vulnerability and adaptation assessments by each province and territory to identify opportunities to decrease risks to health.
Increased surveillance and monitoring of climate-related diseases, and evaluation of the efficacy of adaptation and GHG mitigation interventions.
Provide data that can alert stakeholders in real or near-real time to emergencies as well as provide data for understanding long-term trends.
Program and policy development
A national “Trees for Health” campaign (e.g., trees planted for patients and caregivers at health care facilities).
Funding for sustainable health sector infrastructure.
Guidance on standards for building codes and zoning regulations for the health sector.
Actions to increase health co-benefits of GHG mitigation and adaptation efforts to address climate change.
Northern and Indigenous community considerations
Increased actions to address the health challenges and capacity issues Northern and Indigenous communities face from climate change.
Increased collaboration with Indigenous communities to support education efforts, communicate research findings, and support resilience-building.
Communication and information-sharing
Collaborate on climate change and health communications with the health care community and non-governmental organizations.
Increased public health education using evidence-based advice and targeted messaging.
Incorporate information on climate change and health into educational curricula (e.g., health professionals).
Develop a single window to provide easy access to climate change and health communication materials and messages.
Mechanisms for coordination and collaboration
Increase efforts by federal departments and agencies to support:
Improved preparation of communities for emergency response/disaster recovery.
Improved coordination on climate change and health activities among all federal health departments and agencies, provincial/territorial/local health authorities, and Indigenous partners with needed mechanisms (e.g., climate change and health committee, regional working groups, monthly webinars, collaborative research projects).
Establish a platform to share best practices across provinces and territories (e.g., tool for open-sourcing plans and policies, guidance on developing adaptation options, checklists to assess vulnerability, economic analysis of actions).
Map initiatives on climate change and health and provide funding to support needed actions.
Work more closely with U.S. agencies on climate change and health, taking into consideration important cross-border agreements (e.g., air quality, water quality).
Progress has been made in some of these areas. For example, since 2007, Health Canada has led a heat-health program that is providing support and guidance to local, provincial, and territorial health authorities to develop HARS to protect Canadians from extreme heat events. The program provides public health authorities with guidance on assessing heat-health vulnerabilities at the community level, and on developing heat alert protocols, community response plans, and communications plans. To communicate heat-health risks to Canadians, including to those most vulnerable to the impacts, Health Canada has developed information brochures, infographics, and videos (Health Canada, 2020a; Health Canada, 2020b; Health Canada, 2020c; Health Canada, 2021). Health Canada has also collaborated with a number of communities in Ontario (Windsor, Ottawa, London, and the Regions of Peel and York) and British Columbia (Vancouver) on innovative projects to reduce the urban heat island effect, thereby reducing people’s exposure to higher temperatures in urban areas. The projects helped inform development of a guide for public health officials in Canada on how to engage with partners to address effects of urban health islands on health (Health Canada, 2020d).
Through the HealthADAPT program, launched in 2019, Health Canada is providing funding, information, and expertise to 10 local and regional health authorities across Canada to help build their capacity to understand climate change impacts on populations, develop needed adaptation actions, and communicate with the public and stakeholders on these issues. Many of the projects are examining current and future projected climate change impacts associated with extreme weather events, including on mental health (Health Canada, 2019). Project results and learnings are being shared through a pan-Canadian community of practice that includes public health officials from all levels of government.
Previous climate change and health assessments documented adaptation options for protecting health, roles and responsibilities for health adaptation, and measures being undertaken by health authorities in Canada (Séguin, 2008; Berry et al., 2014a). The following sections provide more detailed information on the current state of adaptation in Canada and describe the range of measures being taken at the regional and local level.
10.3.5.1 Adaptation by Regional and Local Canadian Health Authorities
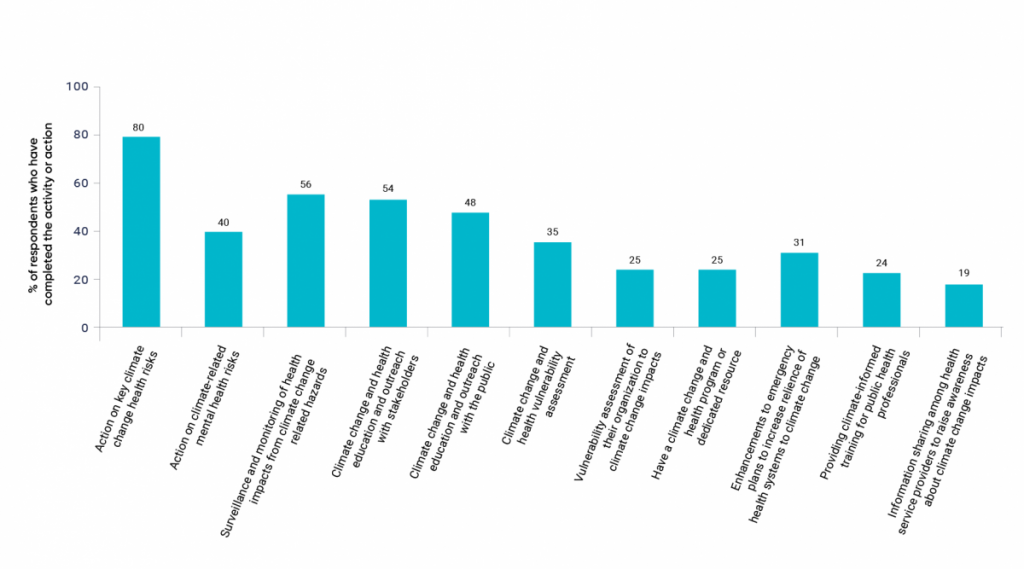
Efforts are underway by a number of Canadian health authorities and partners in other sectors to prepare for climate change impacts on health, including, for example, risks related to extreme heat (Guilbault et al., 2016), extreme weather (Kovacs et al., 2018), and wildfires (Kovacs et al., 2020). A survey of 80 health sector officials from all regions of Canada conducted in 2018–2019 included respondents from Ontario (34), Quebec (11), the Atlantic provinces (7), the Prairie provinces (13), British Columbia (13), and the territories (2). It revealed that large majorities (80% or higher) reported taking some kind of action on health risks of concern due to climate change that were identified in previous assessment reports. These risks of concern included infectious diseases, air quality, extreme heat, other extreme events, and water safety and security, water quality and quantity, and food safety and security. Fewer, but still about four in 10 respondents, indicated they are taking action on climate-related mental health risks (see Figure 10.2) (Survey Research Centre, 2019).
Awareness and groundwork activities and actions on climate change and health undertaken by Canadian health authorities.
Source
Data from Survey Research Centre, 2019.
Many of the activities health authorities have engaged in are awareness-building or groundwork. Just over half of respondents (56.3%) indicated they undertake surveillance and monitoring of the health impacts from hazards related to climate change. In addition, 53.8% reported undertaking climate change and health education and outreach with stakeholders, while just under half (47.5%) have done so with the public. In addition, 35% have undertaken a vulnerability and adaptation assessment for climate change and health, while fewer have undertaken an assessment of the vulnerability of their organization to climate change impacts (25%). Only 21.3% report that they have a climate change and health adaptation strategy, and 10% have a climate change and health research plan (Survey Research Centre, 2019).
Generally, health authorities are undertaking fewer concrete climate change and health actions in response to growing risks to Canadians, and there is a need to quickly scale up effective measures. Only one in four health authorities surveyed reported having a climate change and health program or dedicated resource, and this dropped to one in five for those reporting increasing resources (e.g., funding, human resources) to support adaptation measures (Survey Research Centre, 2019). This suggests that the health programs responsible for protecting the health of Canadians could themselves be vulnerable to climate change impacts and that many health authorities still do not see this issue as a priority, or do not have the resources to address climate issues due to competing priorities. Just over one in three (31.3%) indicated they have integrated climate change requirements into organizational or corporate health standards. Interestingly, 86% of health authorities indicated that they consider the needs of populations at higher risk when developing adaptation strategies. Far fewer consider implications for Indigenous Peoples (37.3%) or the use of Indigenous knowledge and perspectives in such activities (25.4%). Less than one in five (17.9%) consider sex and gender implications when developing measures to reduce climate change risks to health (Survey Research Centre, 2019).
Broader adaptation actions for health system readiness to prepare for climate change are not yet common among Canadian health authorities. For example, only 31% indicated enhancing emergency plans and programs to increase the resilience of the health system and associated health services to climate change impacts (Survey Research Centre, 2019). In addition, just under a quarter (23.8%) reported providing climate-informed training for public health professionals, and just less than one in five (18.8%) shared information among health service providers to raise awareness of possible climate change impacts on staff and/or infrastructure, and to share examples of adaptation options being undertaken. Current levels of education and training activities among Canadian health officials are insufficient to provide them with information needed to proactively prepare for climate change impacts on health (Hacket et al., 2020). New information is available for health authorities and health professionals to use to protect high-risk populations from climate change impacts (see Box 10.4), for example, preparing people with spinal cord injuries for more extreme weather events (Shapiro et al., 2020).
Important limitations of the survey study include the much higher response by health officials in certain regions (Ontario versus the territories and Atlantic provinces) and challenges in accurately identifying officials responsible for climate change and health activities in health authorities.
Another study of public health unit officials in Ontario in 2016 revealed similar results. In particular, 61% of respondents (representing 26 of 36 health units that participated) indicated that they are undertaking activities to raise awareness of climate change impacts on health or of the need to reduce GHGs. As well, 42% reported monitoring climate hazards such as extreme weather, but only 19% indicated they are monitoring climate change impacts on health. One-half of respondents confirmed being involved in research on climate change and health, with 38% indicating their health units have undertaken a climate change and health assessment. Similar to the national survey, but with somewhat higher proportions, 42% of health units reported using a health equity lens to identify, prioritize, and address climate change health risks (Doyle et al., 2017).
Researchers in Quebec have also examined the level of climate change and health adaptation in that province through the Quebec Observatory for Adaptation to Climate Change. For a number of concrete adaptations that help prepare for climate change impacts, health officials in that province are taking more action. For example, 64% (nine of 14) public health departments offer training to staff on climate change and health. In addition, 67% have developed prevention plans to reduce risks from extreme heat and 56% have done so for floods. However, many public health departments are still in the stages of early adaptation, as they are just beginning to allocate budget specifically to adaptation and to develop collaborations with partners in and outside of the health sector (e.g., school boards, community organizations, Hydro Québec) (Valois et al., 2018).
Many health authorities in Canada have not sufficiently scaled up climate change and health adaptation efforts to protect Canadians from current climate variability and from more severe impacts. Significantly ramped-up efforts are needed to train health care professionals, monitor climate change impacts and the effectiveness of adaptation measures, prioritize adaptation with sufficient resources, educate the public and stakeholders, and integrate considerations and information about higher-risk populations into activities.
10.3.5.2 Health in Climate Change Plans and Strategies
Many jurisdictions, from local to national levels, in Canada have climate change plans or strategies that include adaptation, and a greater number now include actions to protect human health and well-being (Kuchmij et al., 2020). Table 10.4 highlights that most provincial or territorial plans now include some reference to human health impacts. However, there is wide variation in the climate change and health activities by health authorities at all levels. Most Canadian provinces and territories are still in the early stages of adapting to the health impacts of climate change, with responses still being fragmented (Austin et al., 2016).
Currently, few provinces and territories have comprehensive or substantive (e.g., covering a wide range of likely risks to health) actions to address climate change and health adaptation as part of their broader climate change strategies. Few jurisdictions have a separate action plan or strategy that focuses exclusively on climate change and health. Given that analysis in other chapters of this assessment suggest wide-ranging health risks and vulnerabilities in communities across Canada, the lack of comprehensive strategies, and the wide diversity and inconsistency of health adaptation planning among many health authorities, increase the vulnerability of Canadians to current and future projected impacts on health.
Table 10.4
Examples of Canadian climate change strategies, action plans, and reports that include human health
Jurisdiction
Strategy/action plan/framework
Examples of health risks and/or determinants of health
Completed emergency evacuation plans for each major territorial health-related facility, and clean air shelter assessments for all but one community to provide safe zones for extreme events such as wildfires
Heat; air quality; vector-borne diseases; food; water quality; forestry; Indigenous communities
Healthy Environments and Climate Change Guideline (2018) to support the Ontario Public Health Standards: Requirements for Programs, Services, and Accountability
Temperature-related morbidity and mortality; natural hazards; air; water quality; food safety and security; zoonotic diseases; extreme heat; sun exposure
Interactive air quality map that increases understanding of air pollution, including wildfire smoke, and provides advice for reducing risk
Climate Change Adaptation Plan to help municipalities learn about climate adaptation, assess how vulnerable they are to events like floods, droughts and severe storms, and build adaptation plans
Climate projections for emergency management; coastal erosion; flooding; infrastructure resilience; water resource management
Province-wide climate change risk assessment to include public health and safety
Source: Adapted from Kuchmij et al., 2020
10.3.5.3 Learning from the Quebec Experience
As a leader on health adaptation, the province of Quebec and its health authorities have been preparing for climate change impacts for almost 20 years (Demers-Bouffard, 2021). A formal requirement to prevent and mitigate the impacts of climate change on public health and safety was included in the Plan d’action sur les changements climatiques (PACC 2006-2012), led by the Quebec Ministère de l’environnement.
In 2012, the Government of Quebec adopted its Plan d’action 2013-2020 sur les changements climatiques (PACC 2013-2020) and the accompanying Stratégie d’adaptation aux changements climatiques 2013-2020, spending $200 million on adaptation (Government of Québec, 2012a; Government of Québec, 2012b). These include several adaptation objectives related to human health, including:
considering climate change adaptation in land-use planning and other planning decisions;
reducing risks and mitigating the consequences of disasters related to climate change;
preventing excess diseases, injuries, and mortality associated with climate change;
maintaining continuity of health and emergency services during disasters related to climate change; and
limiting the psychosocial impacts of climate change.
Through this plan, $22 million was allocated to prevent and limit diseases, injuries, mortality, and psychosocial impacts (Demers-Bouffard, 2021). Led by the INSPQ and with the participation of many partners, a range of adaptation and knowledge development measures have been implemented by the existing Quebec health network. These include an observatory assessing the population’s level of adaptation to climate change; a multi-stakeholder zoonotic observatory; a weather and health warning and monitoring system; emergency response plans; an allergen-pollens reduction strategy; comprehensive research programs on climate change impacts and adaptations; several dozen urban greening pilot projects; and several knowledge transfer tools (websites, online courses, manuals, toolkits for surveys and evaluations, etc.). For example, the INSPQ, along with other partners, launched a Massive Open Online Course on climate change and health for health and social service professionals and for the general public. Other more targeted training is available for doctors, nurses, park workers, and other professions. The Mon climat, ma santé and MSSS websites provide information on the effects of climate change on health, populations at increased risk, and adaptation measures. Detailed clinical guidance is available to physicians for treating illnesses and diseases related to climate change and health in their daily practice (Gosselin et al., 2021).
An evaluation of efforts in Quebec to address climate change impacts on health identified important factors that facilitate such efforts and those that can act as barriers. Factors that supported climate change and health adaptation progress included (Demers-Bouffard, 2021):
major extreme weather events;
prioritization of climate change in government planning;
funding for targeted actions;
clarity of the roles and responsibilities of each of the stakeholders;
availability of local climate and population data; and
identification of external resources to support actions.
Important barriers to protecting health effectively included:
public health resources being monopolized for other priorities;
competition with other public health issues;
organizational focus on the health protection role;
lack of reliable and consistent funding;
ambiguity of roles and responsibilities; and
lack of guidance on the various adaptation measures to be implemented.
Ultimately, political, legal, social, regional, and organizational contexts matter for ensuring that government and regional health authorities can act to adapt to climate change. The political and legal contexts empower the health sector to respond to climate change by providing objectives and resources, while the social and regional contexts influence the development of partnerships and the effectiveness of implementing adaptation measures. The organizational context makes it possible to take advantage of the opportunities provided (Demers-Bouffard, 2021).
10.3.5.4 Individual-Level Health Adaptation
Individual Canadians have a primary responsibility for adapting to the health impacts of climate change by adopting protective behaviours. Educating the public and health professionals about climate change impacts on health is a key function of public health officials, and greater efforts are required to reduce risks (Hathaway & Maibach, 2018). Efforts in and outside of Canada to communicate climate change risks and get people to take protective behaviours have had mixed success and have faced significant challenges (MacIntyre et al., 2019; Maibach, 2019). Many Canadians are aware of climate change impacts on health and concerned about these impacts. In 2017, a survey of Canadians found that 79% of people reported being convinced that climate change is happening, and, of these, 53% indicated that it is a current health risk and 40% believe it will be a health risk in the future (Environics Research Group, 2017). However, concern about impacts is not translating into the adoption of protective behaviours; large numbers of Canadians are not taking actions to protect themselves, or their family members, from climate change impacts on health, putting themselves at higher risk. For example, the survey in 2017 revealed that (Environics Research Group, 2017):
43% of Canadians reported that they had taken steps in the past year to protect themselves and family members against the bite of an infected mosquito or tick (e.g., using insect repellent, wearing long pants and long sleeves, checking for ticks on skin after being outdoors);
37% reported that they had an emergency household plan for what to do during a natural disaster or emergency, down from 42% that reported having one in 2008;
77% reported that they regularly (51%) or occasionally (26%) check for extreme weather alerts, which is down from 2008 when 81% reported doing so;
53% reported that they either regularly (21%) or occasionally (32%) change daily routines as a result of an extreme weather alert; and
51% reported ever having taken action or changed plans as a result of hearing a heat warning.
Interestingly, when respondents were also asked a separate, more general question about whether they had taken steps in the past year to protect themselves or family members from the potential health risks or impacts of climate change, only 37% indicated that they had done so. There were very low rates of reported actions for some possible health adaptations, such as watching the weather more closely (5%), installing air conditioning (2%), having an emergency kit/plan (1%), preparing for storms (1%), and being vigilant for ticks on person/pets (1%) (Environics Research Group, 2017). The difference in responses suggests that many Canadians do not associate these measures with interventions that can protect them from climate change health impacts. In addition, some of the responses to this more general question included “better eating habits/gardening,” “recycling,” “increasing a home’s energy efficiency,” and “driving less,” which are actions to reduce GHGs. Although better home insulation and driving less can help reduce urban heat islands and attendant health risks, there is likely significant confusion among the public of the difference between some GHG mitigation and health adaptation measures.
The media plays an important role in influencing public perception of climate change risks and in influencing behaviours to address climate change (Watts et al., 2018; King et al., 2019). Callison and Tindall (2017) suggested that media coverage of climate change in Canada has tended to focus on national policy making and energy and economic issues, but has often omitted climate justice considerations, including those related to Indigenous Peoples and impacts in the Arctic. A review of climate change impacts on health covered by Canadian newspapers between 2005 and 2015 suggested that coverage over this time period has actually decreased, with greater information being provided to the public on negative climate change impacts on health and significantly less on climate change and health adaptation solutions. In fact, only 26% of the articles reviewed included information on actions that can be taken to protect health (King et al., 2019). The authors suggest that recent trends in media coverage of climate change in Canada may be partly responsible for a lack of public support and actions to address climate change, including preparing for the impacts (King et al., 2019). Adaptation by individual Canadians may also be significantly influenced by constraints on their ability to take protective actions due to existing inequities in society (see Chapter 9: Climate Change and Health Equity).
10.4
Health System Vulnerability and Resilience to Climate Change Impacts
Share
10.4.1
Health System Vulnerability
Share
A range of impacts from extreme weather events and public health emergencies related to climate change can affect health facilities and systems (WHO, 2015; Balbus et al., 2016; Curtis et al., 2017; Ribesse & Varangu, 2019). The ability of these systems to mitigate climate change impacts on populations will be increasingly challenged in the future (Ebi & del Barrio, 2017). For example, cancer care can be disrupted by climate-related disasters that affect infrastructure, communications systems, availability of medications, and medical records (Man et al., 2018). The Lancet Countdown on Health and Climate Change suggested that health systems are unprepared to manage the impacts of climate change. Specifically, it reported that “A lack of progress in reducing emissions and building adaptive capacity threatens both human lives and the viability of national health systems they depend on, with the potential to disrupt core public health infrastructure and overwhelm health services” (Watts et al., 2018, p. 2479). Globally, between 2005 and 2019, an average of 412 health facilities were damaged or destroyed by climate-related disasters annually, and such impacts are increasing (UNDRR, 2019). Many decision makers expect climate change to worsen these risks; a survey of 814 global cities in 2019 indicted that 67% of respondents believed that climate change would seriously affect their public health assets and infrastructure (Watts et al., 2021).
Health care officials, including first responders, can be affected physically and suffer mental health impacts from extreme weather and disaster events. Health infrastructure, such as building envelopes, can be damaged or destroyed by wind storms, floods, wildfires, and extreme heat events. Reduced access to critical support services, including transportation, power, water supply, and telecommunications, can affect the normal operations of a health care facility (Scott et al., 2020; WHO, 2020). Medical and non-medical supplies and services (e.g., medications and medical products, blood services, food, linen and site cleaning, waste disposal storage and services, data management and patient record systems, and sterilization services) can be disrupted by severe weather events in or even outside of Canada. Patient safety can be compromised when access to critical health and clinical services, such as surgery or radiation therapy (Xiu-Gee Man et al., 2018), are reduced or when outpatient services, such as dialysis, are affected.
During disasters, increased hospital admissions and emergency services in health facilities can create stress on operations, particularly where surge capacity is lacking, where there are ongoing requirements for medication or treatment, and when patients are transferred from other affected facilities (Ebi et al., 2017; WHO, 2020). The activation of the emergency plan within the health care facility is a significant undertaking, and health care facilities experiencing climate change-related impacts will incur increased costs (Ribesse & Varangu, 2019).
Climate change is expected to increase future risks to health facility and health system staff, operations, and infrastructure in Canada from a range of hazards (Ribesse & Varangu, 2019). Some hazards, such as flooding, could affect critical health infrastructure, leading to severe health and socio-economic impacts on Canadians (Scott et al., 2020). Scott et al., (2020) examined the risks to health and emergency facilities (e.g., hospitals, long-term care centres, outpatient clinics, community health centres, police, fire) from floods due to river overflow, extreme rain events, and storm surge. Across Canada, 15.2% (17,177) of all health and emergency facilities (112,910) have some exposure to flood hazards, increasing their vulnerability to the impacts of this type of extreme event. Health care services constituted 94% or 16,240 of the health and emergency facilities that are at risk (Scott et al., 2020). In addition, a study of the climate resilience of facilities at Fraser Canyon Hospital in Hope, British Columbia, found that elevated temperatures are already being observed in the buildings. The projected quadrupling of hot days (>30°C) between 2016 and 2050 due to climate change will exceed the capacity of the heating, ventilation, and air conditioning (HVAC) systems to maintain thermal comfort, necessitating retrofits, such as building envelope upgrades and horizontal shading elements above windows (Bartko & Macdonald, 2017).
Discernable effects of climate change on health and on health systems are already evident and will increase in the absence of efforts to address existing vulnerabilities and close the “health adaptation gap” (Martinez et al., 2018; Haines & Ebi, 2019). In the United States, Superstorm Sandy, which struck in November 2012, severely affected health services in New York, with 3.1 billion USD in recovery costs (Health Care Climate Council, 2018). Health facilities in Canada are already being affected by climate hazards (Waddington et al., 2013; Canadian Coalition for Green Health Care, 2019b). Health authorities have reported impacts of climate-related events on the following health facility functions: damage to infrastructure, reduced access to medical supplies and products, reduced access to critical support services (including transportation, power, water supply, and telecommunications), and activation of emergency services (Canadian Coalition for Green Health Care, 2019b).
Table 10.5 provides information on Canadian health facility vulnerabilities to specific climate change hazards. It includes examples of climate-related impacts on health facilities. As there is no comprehensive and centralized surveillance system for monitoring such impacts, these types of impacts are likely significantly under-reported.
Table 10.5
Canadian health facility vulnerabilities to climate change hazards
Climate hazard
Potential impacts on health facility
Examples of vulnerability/risk factors
Examples of impacts on Canadian health facilities
Temperature extremes: extreme heat events including longer periods, hotter nights, and high humidity
Disruption/closure of specific departments (e.g., operating theatres)
Patient transfers
Increased patient admissions
Increased mortality and therefore strain on morgue use
Patients, staff, and visitors require safe temperatures to maintain good health
Some medical services and procedures (e.g., operating theatres) require temperature and humidity levels to be maintained within specific levels
Warmer temperatures bring increased risk of food-, water-, and vector-borne diseases
Influx of community members to hospitals for use as cooling areas
Royal Victoria Hospital, Barrie, Ontario, 2019: Heat and humidity caused the air conditioning to break down in the older portion of the hospital, forcing the cancellation of 130 non-emergency surgeries, patient transfers, resterilization of medical equipment and linens (CTV Barrie, 2019)
Nine health regions in Quebec, 2018: A period of extreme heat resulted in 86 excess deaths reported. Significant increases in hospitalizations, ambulance transports, and emergency admissions observed in several regions. Lack of air conditioning in patient rooms caused concern for patient health (Poitras, 2018).
Eight health regions in Quebec, 2010: July 2010 heat wave resulted in a significant increase in emergency department admissions (4%) and 33% increase in death rates for all of the health regions affected.
Toronto, Ontario, area hospitals, 2002–2010: A 29% increase in emergency room visits for specific mental and behavioural diseases was observed over a cumulative period of seven days after exposure to high ambient temperature (mean daily temperature of 28°C or higher).
Regina General Hospital, Regina, Saskatchewan, 2007: Operating theatre closed for eight days due to high heat and humidity levels.
Temperature extremes: cold snaps, including ice storms and extreme snowfalls
Disruption/closure of specific services and departments (e.g., operating theatres)
Patient transfers
Increased patient admissions
Power outages
Staff shortages
Disruption to transportation networks
Shortages of blood supplies
Influx of community members to hospitals for use as warming areas
Energy systems in health facilities can be affected by cold snaps and ice storms
Winter storms can affect transportation networks vital for the functioning of health care facilities
Eastern Health, St. John’s, Newfoundland and Labrador, 2020: Extreme snowfall resulted in the City of St. John’s declaring a State of Emergency for eight days. Emergency and urgent services at five health facilities in St. John’s were delayed, while all other services at these sites were cancelled for a few days. Closures also included family doctor and specialty clinics, pharmacies, outpatient blood collections, and interruptions in patient services, such as appointments, procedures, and surgeries; some health professionals stayed on the job for 60 hours.
Sunnybrook Health Sciences, Toronto, Ontario, 2013: A power grid failure from an ice storm lasted 39 hours. Emergency power enabled continued activity in trauma bays, emergency rooms, and intensive care units. However, some less critical services to patients were affected — medical imaging appointments were cancelled, lab tests were delayed, food delivery to inpatients was delayed, retail food operations were without power, and computer networks and email systems were disrupted. As a precaution, six infants in the Neonatal Intensive Care Unit were relocated to other hospitals. Community members gathered in the hospital for warmth (Canadian Coalition for Green Health Care, 2017).
Flooding caused by extreme rainfall, river flooding, freezing water pipes, and storm surges resulting from hurricanes
Transfer of patients from affected health care facilities
Staff shortages due to health impacts and disruptions to transportation routes
Boil water advisories
Power outages
Disruption/closure of specific departments (emergency, clinics)
Infrastructure damage (roof being torn off due to high winds)
Internal flooding, including basements
Mental health impacts on staff
Shortages of blood supplies
Damage to medical equipment
Hurricanes, storm surges, and flooding can damage critical health facility infrastructure and interrupt supply chains for food, water, energy and medical supplies
During weather emergencies, roads may be destroyed or closed to discourage travel
Post-event or post-disaster clean-up can reduce or prevent access to health care facilities
Impacts on blood donations by the public
Physical and mental health of health facility staff can be affected by floods
Hotel-Dieu of St. Joseph Hospital, Perth-Andover, New Brunswick, 2012: Flooding by more than 1 m of water led to the temporary closure of the hospital and the transfer of 21 patients to other facilities (Canadian Broadcasting Corporation, 2012; Government of New Brunswick, 2012). Construction of a new essential services building was part of a $7.65 million investment to restore, preserve, and protect critical infrastructure at the hospital (Government of New Brunswick, 2018).
Kings County Memorial Hospital, Montague, Prince Edward Island, 2010: Heavy rain and a malfunctioning roof drainage system resulted in water coming in through the ceiling. The emergency department was shut down, and cases were diverted to the Queen Elizabeth Hospital in Charlottetown (Canadian Broadcasting Corporation, 2010).
Quebec hospitals around Montréal, Quebec, 2017: Flooding in the cities of Montréal and Laval resulted in evacuation of three health care centres (Presse Canadienne, 2017). Patients also had to be transferred from a long-term care centre (Canadian Broadcasting Corporation, 2017). The Ministry of Health and Social Services provided psychosocial support services throughout Quebec (Presse Canadienne, 2017).
Winnipeg Health Sciences Centre, Manitoba, 2014: Storm rain resulted in basement flooding of the Ann Thomas Building, which housed the medical device reprocessing area. In addition, numerous equipment storage rooms were flooded and patient food services were affected, resulting in service delays for patients and visitors. The incident did not create any surgery delays, given the ability of the department, maintenance, and cleaning crews to work through the night to remove water, repair ceilings, and reprocess supplies (Canadian Coalition for Green Health Care, 2015a).
Alberta Health Services Facilities, Alberta, 2013: Floods resulted in evacuations, isolations, and/or damage to multiple hospitals, urgent care centres, continuing care and long-term care sites, as well as Alberta Health Services corporate, community, emergency medical services facilities, and physician offices (Alberta Health Services, 2013a; Canadian Broadcasting Corporation, 2013; MNP LLP, 2013; United Nurses of Alberta, 2013; Alberta Health Services, 2014; Watts, 2014). More than 1000 patients were evacuated in the Calgary Zone in the first 24 hours (Alberta Health Services, 2013b). Staff were displaced from places of work, and many had their own homes damaged or destroyed (Watts, 2014). A number of flood-related boil-water orders were issued across the province (Alberta Health Services, 2013a). Mobile mental health teams were dispatched to High River to facilitate access to services and provide mental health support (Alberta Health Services, 2013b).
Hurricane Maria, Puerto Rico, U.S., 2017: Hurricane Maria caused global shortages of medical supplies. The destructive forces of hurricanes can have a dual impact on health care facilities — first, they have physical impacts on the local facilities and the resources they require (Panditharatne, 2018), and, second, they can have an impact on global supply chains for medical products (GEP, 2017; Kodjak, 2017). Widespread devastation of the critical infrastructure, including power and water supplies, resulted in manufacturing challenges (GEP, 2017; Kodjak, 2017). Puerto Rico is home to over 50 medical device manufacturers and over 80 pharmaceutical manufacturers (GEP, 2017) that supply products to Canadian hospitals.
Extreme winds, including those caused by tornadoes and hurricanes
Interruptions to information technology and communications
Transfer of patients from affected health care facilities
Staff shortages due to health impacts and disruptions to transportation routes
Increase in admissions
Boil water advisories
Disruption/closure of specific departments (emergency, clinics)
Infrastructure damage (roof being torn off due to high winds, basement flooding)
Mental health impacts on staff
Shortages of blood supplies
Power outages
Tornadoes can damage critical health facility infrastructure and interrupt supply chains for food, water, energy, and medical supplies
During weather emergencies, roads may be destroyed or closed to discourage travel
Post-event or post-disaster clean-up can reduce or prevent access to health care facilities
Physical and mental health of health facility staff can be affected by severe storms
Nova Scotia Health Authority, Nova Scotia, 2019: Hurricane Dorian generated high winds, causing power outages at many hospitals and service locations, which had to operate on emergency generator power. Some sites experienced additional impacts, including phone, internet, and network issues; water damage; temporary closures; and cancellation of patient appointments and procedures (Nova Scotia Health Authority, 2019a; Nova Scotia Health Authority 2019b).
Victoria General Hospital, Halifax, Nova Scotia, 2003: High winds from Hurricane Juan created power outages and tore off parts of the hospital roof, requiring the evacuation of 51 patients. The event left the entire health care system with a backlog of hundreds of operations and appointments. Transportation issues complicated the work of Emergency Health Services, and Public Health Services were concerned with monitoring food and water safety and the possible spread of communicable diseases (Globe and Mail, 2003; Nova Scotia, 2003).
Memorial Hospital, Sudbury, Ontario, 1970: Tornado winds in the city resulted in six deaths, 200 injured, and hundreds left homeless. The winds ripped off the roof of a partly completed wing of the Memorial Hospital (Commito, 2018).
Wildfires
Transfer of patients from affected health care facilities
Staff shortages due to health impacts and disruptions to transportation routes
Boil water advisories
Disruption/closure of specific departments due to air contamination (e.g., emergency, clinics)
Infrastructure damage (roof torn off by high winds, basement flooding)
Mental health impacts on staff
Shortages of blood supplies
During wildfires, roads may be destroyed or closed to discourage travel
Post-event or post-disaster clean-up can reduce or prevent access to health care facilities
Physical and mental health of health facility staff can be affected by wildfires
Interior Health, British Columbia, 2017: Wildfires resulted in air quality warnings due to very high health risk from the smoke, and in the temporary closure of 19 health care facilities or sites. Additionally, 880 patients were evacuated from facilities, and more than 700 health services staff displaced, with a total cost to the health authority of $2.7 million. Many patients were evacuated to neighbouring Northern Health facilities, straining health care resources in Kamloops and Prince George (Canadian Healthcare Facilities, 2017; Interior Health, 2017).
Northern Lights Regional Health Centre, Fort McMurray, Alberta, 2016: A wildfire resulted in 73 acute care patients, including nine babies in the neonatal unit and their mothers, and 32 continuing care patients who were wheelchair-bound, being moved to three different reception areas outside Fort McMurray via ambulances and buses (Warr, 2016). Alberta Health Services reserved 92 hotel rooms in Edmonton for the health care workers attending to these patients. Other impacts on the hospital included smoke damage and air quality concerns (Drinkwater, 2016; KPMG, 2017).
Landslides and avalanches
Interruptions to information technology and communications
Transportation routes blocked
Medical operations are postponed
British Columbia, 2020: Rockslides after heavy rain damaged cell towers, which caused widespread disruptions to phone service across British Columbia, including communications with health care staff (Boynton, 2020).
Melting permafrost
Building infrastructure destabilized
Transportation routes (including airstrips) built on permafrost are unstable; winter ice roads less reliable
Damage to pipelines and power lines
Health care facilities and other health system buildings require stable ground
Canadian Arctic: Rising temperatures in the Far North are melting permafrost, requiring a number of health care facility buildings to be structurally supported with thermosyphons to prevent them from sinking (Holubec, 2008).
Source: Adapted from Balbus et al., 2016, with data from the Canadian Coalition for Green Health Care, 2020
Climate impacts are not all acute events. Impacts can be less drastic and longer-term, but such cumulative impacts can also be significant. More frequent rainfall or gradual increase of day- and night-time temperatures and humidity levels can strain the physical plant (i.e., air conditioning and ventilation systems) while increasing the need for health services (i.e., more patients with heat stress). As another example, permafrost melt in Canada’s Far North is damaging the foundations of some medical clinics, and continued warming will require remediation to prevent further damage to these structures (Holubec, 2008). Permafrost maps were developed for health authorities in Nunavik to guide future decisions about planning new buildings and renovating those at structural risk by thawing (L’Hérault et al., 2013).
Climate hazards can also combine, or cascade, as happened in Dunrobin, Ontario, which was affected by record flooding in 2017, devastating tornadoes in 2018, and further severe flooding in 2019. Similarly, flooding in Japan in 2018 killed more than 200 people and was followed during the clean-up efforts less than a month later by record-breaking extreme heat that resulted in at least 30 deaths and 10,000 hospital admissions (ABC News, 2018). Whether acute climate shocks or chronic stresses, climate impacts will require health systems to respond and adapt (Ebi et al., 2018b).
Impacts on health systems in Canada can be very severe, as was the case with the 2013 Southern Alberta floods, when some hospitals were forced to close, patients were evacuated, and significant infrastructure damage occurred (MNP LLP, 2013; Roles, 2013). The catastrophic wildfires in British Columbia in 2017 and 2018 also resulted in facility closures, patient transfers, and major disruptions to care (Legassic, 2018). Climate events can have disproportionate impacts on Indigenous communities. For example, almost 2000 people displaced from four First Nations communities in Manitoba after extensive flooding in 2011 were still unable to return to their homes in 2017 (Lambert, 2018).
A major challenge facing health systems in Canada from climate change are possible surprises or unexpected hazards, events, or developments; these present new or much more severe threats to the health of Canadians or to health systems. For example, significant uncertainty exists about the impacts of climate change on human migration, and very little research has been conducted in the Canadian context. However, some evidence suggests that climate change could lead to large movements of populations seeking respite from climate-related disasters and other impacts. A U.S. National Intelligence Council study warned that climate change will continue to threaten the stability of many countries through climate-induced disruptions that can overwhelm response capacity (NIC, 2016). Missirian and Schlenker (2017) suggest that, under a high emissions scenario, the European Union could see annually an additional 660,000 asylum applications by the end of the century, a 175% increase from the present day.
Evidence suggests that many health facilities — a critical component of health systems in efforts to reduce climate change impacts — are not taking needed actions to prepare for current risks and future warming. A survey of health care facility staff, such as facility directors or managers, sustainability coordinators, and energy managers, representing 102 facilities, was undertaken by the Canadian Coalition for Green Health Care in 2019 through the Green Hospitals Scorecard questionnaire (Canadian Coalition for Green Health Care, 2019b). The respondents were primarily located in Ontario but also at some facilities in British Columbia, Manitoba, and Nova Scotia. The survey revealed that health authorities are recognizing climate change as an issue of concern, and some are taking adaptation measures. For example, 55% reported that senior leadership had assigned at least one person with some climate change responsibility in their health authority. However, only a small percentage of health care facilities (8%) had acknowledged climate change in their strategic plan or had identified climate risks in specific policies. A smaller number of facilities (4%) reported that the impacts of climate-related events, such as flooding and severe weather events, had been recognized in other ways. In addition, almost one-third (27%) of facilities had not recognized climate change as an issue of concern, and 10% responded that they did not know whether it was an issue of concern (Canadian Coalition for Green Health Care, 2019b).
Awareness of the need to examine the possible impacts of climate change on health facilities is relatively new. Therefore, few health facilities in Canada have undertaken assessments of vulnerability or have a good understanding of what vulnerability assessments would entail. Of the health care facility staff respondents (99 respondents), 9% reported having completed resilience assessments, while only 4% had completed vulnerability assessments (Canadian Coalition for Green Health Care, 2019b).
Use of on-site renewable energy systems can improve the resilience of the health care facility during grid-based power outages and reduce the generation of GHGs from the use of fossil fuels. Just over a quarter (27%) of health care facilities reported that they currently had some form of renewable energy in place, with many reporting multiple types of systems (100 participants provided multiple responses for a total of 245) (Canadian Coalition for Green Health Care, 2019b). Of the renewable energy systems currently in place, photovoltaic systems are currently the most popular (9%), followed by deep lake cooling (4%), with other numerous renewable energy system types at much smaller numbers. The potential growth of renewable energy systems in the future is significant, with 46% hoping to implement some renewable energy options in the future (Canadian Coalition for Green Health Care, 2019b). The renewable energy types of highest future interest are photovoltaic systems (45%), geothermal systems (14%), deep lake cooling (13%), and solar hot water (12%) (Canadian Coalition for Green Health Care, 2019b).
Given that the health system and health facilities are the first and last defence from climate change impacts on the health of Canadians, the limited number of existing efforts to build health facility resilience across Canada and educate and train health officials suggests ample opportunity to reduce existing vulnerability to health impacts.
10.4.2
Economic Impacts of Climate Change Effects on Health and Health Systems
Share
When climate change increases mortality or morbidity, there is a loss of welfare to society and forgone income and/or wealth creation. Climate change may also disrupt labour productivity, educational attainment and other determinants of health, eroding economic output and future potential. Although limited evidence is available, climate change-driven impacts to various economic sectors (e.g., resource extraction) may disrupt future government revenues, including those that fund health and social services. In addition, more illnesses, injuries, and disease may increase stresses and costs to health systems and result in general impacts on economic productivity, with more sick leave and absenteeism (Campbell-Lendrum et al., n.d.; Martinez et al., 2018). To manage growing health risks effectively, decision makers need to know the following information about adaptation options: (1) the economic costs of climate change impacts on health in the absence of interventions; (2) the costs of implementing adaptation actions to protect health, including measures in and outside of the health sector; and (3) the costs of health impacts that are residual or that still occur after actions are taken (Campbell-Lendrum et al., n.d.).
There is a paucity of information about the economic costs of current climate variability and projected climate change on the health of individuals and on health systems internationally (Hutton & Menne, 2014; Martinez et al., 2018) and in Canada (Berry et al., 2014a). However, climate change is expected to result in tangible and significant economic costs to health systems and broader society (Kovats et al., 2011; Watkiss, 2015; Ebi et al., 2017).
Projections of future economic costs of climate change on health are uncertain and vary widely, depending on availability of data and methods used. The WHO has projected that a narrow range of direct climate change impacts on health would result in economic costs of 2 billion to 4 billion USD by 2030 (WHO, 2018b). Another study, with a broader set of health outcomes and including indirect costs, suggested that European Union countries alone might expect health costs between EUR 9 billion and 106 billion for the period 2041–2070 (Ciscar et al., 2014). In the United States, one study estimated the health costs of 10 climate-sensitive events that struck in 2012, including heat waves, hurricanes, wildfires, flooding, outbreaks of infectious diseases, and ozone pollution. The total cost was at least 10 billion USD, related to 900 deaths, 21,000 hospitalizations, 18,000 emergency room visits, and 37,000 outpatient visits (Limaye et al., 2019). The very severe wildfires in Washington and Colorado in that year resulted in 419 deaths and 627 hospital admissions, for a total cost of 3.9 billion USD (Limaye et al., 2019).
Recent research in Quebec suggested that, from 2015 to 2065, the projected costs of the increase in health effects of ragweed allergies due to climate change are $360 million for governments in that province and $475 million for society as a whole. For extreme heat, the study estimated costs of $370 million for governments and over $33 billion for society. In addition, increases in Lyme disease due to climate change are projected to cost governments $60 million to $95 million, depending on the level of public health preparation (Larrivée et al., 2015).
The health care costs will not be borne evenly among the population. For example, evidence suggests that the most vulnerable in society bear disproportionate health care costs from the impacts from extreme heat (Wondmagegn et al., 2019). Box 10.5 describes the health system impacts and economic costs of recent severe wildfire seasons in British Columbia.
Some of the costs to health and health care systems from climate change are avoidable through adaptation, but these actions often require upfront development and subsequent maintenance costs. Greater research is needed on the costs and benefits of various adaptations to reduce risks to Canadians from extreme heat and other climate change hazards.
10.5
Climate-Resilient Health Systems
Share
Because of the increasing severity and frequency of climate-related emergencies and disasters, health authorities need to prepare health and emergency services to be able to respond during such events (UNDRR, 2015; Watts et al., 2018; WHO, 2018c). Strengthening health systems is a “no-regrets” strategy that can reduce climate risks while also protecting health from other global challenges, such as pandemics (Banwell et al., 2018). Human health and well-being are most effectively protected from the impacts of climate change when health authorities take measures to increase the climate resilience of whole health systems (WHO, 2015; WHO, 2018c; Ebi et al., 2019). The “health system” refers broadly to the organizations of people, institutions, and resources that work to protect and promote population health (Ebi et al., 2019), encompassing health care planning, facilities, and services as well as traditional public health functions (e.g., health promotion through social participation and empowerment; disease surveillance and response; emergency preparedness; health research; and health information systems) (WHO, 2015). A climate-resilient health system has the capacity to monitor, anticipate, manage, and adapt to the health risks of climate change to maintain efficiencies and the ability to improve population health, and to reduce inequities and vulnerabilities as climate change impacts increase (WHO, 2015) (Figure 10.3).
Ten components comprising the WHO operational framework for building climate-resilient health systems.
Source
WHO, 2015.
Currently, a number of health authorities in non-governmental organizations, bilateral agencies, and national and subnational ministries of health are using the WHO Operational Framework to build the capacity and information base to mainstream climate change into health policies and programs (Ebi et al., 2019).
There is greater recognition among health authorities that health facilities play a critical role in protecting people from the impacts of climate change, given that they are the last resort for treating illnesses and injuries (WHO, 2015; Balbus et al., 2016; Miller et al., 2018). Health facility officials, and broader health systems, can prepare for climate change impacts and reduce risks from current hazards by (Balbus et al., 2016; WHO & World Bank, 2018; Ribesse & Varangu, 2019):
developing initiatives to become more climate resilient, including adapting policies and processes as needed to meet challenges of the changing climate;
leading by example by reducing GHG emissions while promoting sustainability in the entire medical supply chain;
making health care facilities safer and more environmentally sustainable;
training health personnel to recognize and understand the effects of climate change; and
encouraging health personnel to advocate and act to reduce the carbon footprint and build resilience.
Health systems in Canada have an opportunity to contribute to efforts to slow climate change while increasing resilience to the impacts (Miller et al., 2018). Challenges to adapting to the effects of climate change will be much greater without stronger measures to reduce GHGs (IPCC, 2014). Preparing Canadians for climate change impacts on health requires robust knowledge of risks to health facilities and health care services in the context of broader vulnerabilities facing communities and populations at higher risk. Investigations of health facility vulnerability can provide useful data, including estimates of current and future climate resilience of buildings and clinical services, and information on patient admissions, to understand the needs for improving patient care during climate-related emergencies. For example, Haines and Ebi (2019) suggest that efforts to modify current health policies and measures to protect health from climate change must consider needed adjustments to new building codes and to the optimal location of new buildings, including health facilities, to reduce risks from impacts associated with rising temperatures and flooding.
New assessment tools and methods exist to help officials in health care facilities in Canada undertake studies that gauge their resilience to climate change impacts and inform actions to increase their sustainability (Balbus et al., 2016; Ribesse & Varangu, 2019; BC Health Authorities, 2020). For example, in partnership with Health Canada, the Canadian Coalition for Green Health Care developed a Health Care Facility Climate Change Resilience Checklist (Paterson et al., 2014) that poses questions on emergency management, facilities management, health care services, and supply chain management. The Coalition also delivered a Climate Change Resilience Mentoring Program, which included online learning resources.
In addition, a process to assess the vulnerability of infrastructure to climate-related impacts, known as the Public Infrastructure Engineering Vulnerability Committee protocol, was developed by Engineers Canada in partnership with Natural Resources Canada. This tool guides a review of past climate information to project the nature, severity, and probability of future climate-related events and the impacts of these events on infrastructure, in terms of deterioration, damage, or destruction, to identify higher-risk components (PIEVC, n.d.). This process was applied to the Nanaimo Regional General Hospital in British Columbia, and the report provided information to prioritize components requiring adaptation, as well as to understand the best ways of adapting them, through design adjustments or changes to operational and/or maintenance procedures (RDH Building Science, 2018).
Most local to national vulnerability and adaptation assessments for climate change and health that have been completed in Canada have not examined, or have not included in detail, information on risks and vulnerabilities facing health facilities and adaptation options (Séguin, 2008; Gosselin, 2010; Berry et al., 2014a; Berry et al., 2014b; Levison et al., 2018). Future assessments would benefit from examination of climate change risks to health facilities and the engagement of representatives from the health care sector (Ebi et al., 2018b; Ribesse & Varangu, 2019). In British Columbia, a study by the Fraser Basin Council in 2016 found that a very severe coastal flood (currently a once in 500-year event) could affect three wastewater treatment facilities and 15% of health care facilities, including three hospitals, while displacing approximately 238,000 people (Fraser Basin Council, 2016).
Climate change and health stress-testing of health facilities and other critical parts of the health system can be undertaken as part of broader assessments of disruptive climate-related shocks and stresses that could overwhelm the capacity to respond to these events. Health authorities can use hypothetical scenarios and simulation exercises in workshop settings to learn about possible resilience tipping points affecting facilities to develop and implement appropriate adaptation measures (Ebi et al., 2018b). Stress-testing exercises have been undertaken to examine the resilience of hospitals in Vancouver Coastal Health Authority, British Columbia (Lower Mainland Facilities Management, 2020). Integrating health facility considerations and information in assessments supports broader community preparedness for climate change impacts, given the importance of transportation, power, water, and wastewater services to hospitals during emergencies and the critical role these facilities play in reducing climate-sensitive injuries, illnesses, and diseases in communities (Ribesse & Varangu, 2019).
Resilience indicator categories for health care facilities in Canada that may be used in assessments have been proposed using the WHO Operational Framework (Table 10.6) (Canadian Coalition for Green Health Care, 2018).
Table 10.6
Proposed climate resilience indicator categories for health care facilities in Canada
Proposed health care facility framework components
Proposed health care facility resilience indicator categories
Leadership and governance
Executive responsibility for climate change
Health workforce
Staff awareness and knowledge of climate impacts on health and the health system and of clinical interventions
Workforce preparation for and support during climate events
Readiness to communicate internally and externally on climate change
Coordination and collaboration on climate change with outside agencies
Vulnerability, capacity, adaptation, and resilience assessment
Identification of vulnerabilities to climate change by health care facility
Resilience assessment used to develop Health Care Facility Resilience Plan
Participation in vulnerability and adaptation assessments with local public health and community organizations
Capacity-building plans to address gaps in human resources and institutional capacity
Risk monitoring and early warning
Early warning systems and other tools for extreme weather events and climate-sensitive diseases
Health and climate research
Climate change health research at health care facility
Climate-resilient and sustainable supply chain and supporting logistics
Sustainability and resilience to climate-related impacts considered in selecting products and services
Climate-resilient and sustainable facility infrastructure
Assessment of health care facility’s impact on environment, including carbon emissions
Climate-related impacts included in scoping new construction and development
Use of new technologies to address GHG mitigation, resilience, adaptation, and emergency management
Health impact assessments for new mitigation and adaptation initiatives
Staff awareness of climate impacts on health and the health system
Workforce preparation for and support during climate events
Readiness to communicate internally and externally on climate change
Coordination and collaboration on climate change with outside agencies
Staff awareness of climate impacts on health and the health system
Early warning systems and other tools for extreme weather events and climate-sensitive diseases
Sustainability and resilience to climate-related impacts considered in selecting products and services
Emergency preparedness and management
Emergency management and continuity plan that has a climate change lens and includes actions that anticipate, respond to, cope with, recover from, and adapt to climate change
Emergency management and continuity plan based on stakeholder engagement and collaboration, with community input, buy-in, and approval
Climate and health funding
Resources available and allocated to increase resilience, environmental sustainability, low-carbon mitigation, and adaptation
Source: Adapted from Canadian Coalition for Green Health Care, 2018
Many health sector officials are willing to take actions to prepare health facilities for climate change threats when they have the required information about current and future climate change impacts and vulnerabilities. A snapshot of the types of actions that health care facilities in Canada have undertaken following a climate change resilience assessment was obtained from surveys of participants in the Health Care Facility Climate Change Resilience Mentoring Program (2016–2019). A total of 31 participants from 21 health care facilities took part in this program, with 13 participants from Ontario-based health care organizations, and others from British Columbia, Manitoba, and New Brunswick (Canadian Coalition for Green Health Care, 2019a). The majority (77%) of survey respondents implemented resilience practices in their facilities. These included sharing climate-related assessment reports with colleagues; undertaking infrastructure and equipment upgrades; exploring renewable energy options; instituting new response codes for climate-related impacts; undertaking vulnerability assessments; updating contingency/disaster plan(s) and disaster preparedness supply lists; and providing advice to patients on how to stay safe in extreme heat. Many of the participants also began a discussion of climate change with senior leaders. The reported primary barriers to undertaking climate change resilience assessments were a lack of support from senior leaders and a lack of funds and resources (Canadian Coalition for Green Health Care, 2019b).
Major cost savings may accrue to health care facilities that take actions to prepare for climate change. A study examining a scenario in which a hospital in the United States invested in climate resilience found that it would have stayed operational during a hypothetical strike by a major hurricane, avoiding a revenue loss of 10% (estimated for a facility that did not prepare). It would also have experienced a 5% increase in costs due to minor repairs (versus a 20% increase for an unprepared facility) and saved an overall $100 million thanks to its climate adaptation actions (Health Care Without Harm, 2018).
10.6
Health Co-Benefits of Adaptation and GHG Mitigation Measures
Share
Because GHG mitigation and a range of adaptation measures have the potential to make great strides in advancing population health, the Lancet Countdown on Health and Climate Change suggested that “tackling climate change could be the greatest global health opportunity of the 21st century” (Watts et al., 2015). Well-designed approaches to addressing climate change that engage a wide range of sectors (e.g., energy, water, housing, urban planning, transportation, insurance, agriculture, and food systems) through a “health-in-all-policies” approach9 can result in very large immediate and long-term health co-benefits and cost savings to the health system (Haines et al., 2009; Friel et al., 2011; Jarrett et al., 2012; Cheng & Berry, 2013; Springmann et al., 2016; NASEM, 2018; WHO, 2018b; Hamilton et al., 2021). For example, GHG mitigation and adaptation efforts that significantly reduce fossil fuel use (e.g., changes to the design of transportation infrastructure in communities to improve thermal comfort; use of low-emission vehicles; promotion of active and public transportation) also improve air quality by reducing fine particulate matter, including black carbon and tropospheric ozone; these efforts can have multiple co-benefits, including reductions in cardiovascular and respiratory diseases (see Chapter 5: Air Quality). Greening communities to cool them can also have multiple knock-on health benefits, such as reducing chronic diseases and improving mental health (Health Canada, 2020a), as can other measures to make communities more livable, such as walking and biking paths (Green et al., 2018). These measures can also have positive impacts by reducing social isolation and crime in some neighbourhoods (Beaudoin & Levasseur, 2017). The Government of Canada committed to considering health co-benefits, such as reduced air pollutant emissions, when developing policies and measures to reduce GHG emissions (Government of Canada, 2016).
The value of possible health co-benefits of actions is very large. Non-communicable diseases are estimated to cost $68 billion in health care spending per year (PHAC, 2011 as cited in Chronic Disease Prevention Alliance of Canada, 2017), while insufficient physical activity has been estimated to cost the health system $2 billion in direct treatment costs (Janssen, 2012). Therefore, relatively modest reductions in these diseases through efforts to achieve health co-benefits could reap large cost savings. In the United States, it has been estimated that clean-energy policies to reduce GHGs consistent with the Paris Agreement target could result in lower particulate matter and ozone levels, preventing 175,000 premature deaths by 2030 and approximately 22,000 deaths each year into the future (Shindell et al., 2016). A similar global analysis of health co-benefits from 2020 to 2100 in urban centres included calculations for Toronto (11,000 avoided deaths) and Montréal (4000 avoided deaths) (Shindell et al., 2018). In addition, a health-impact analysis conducted for the introduction of Tier 3 vehicle and fuel standards in Canada in 2015 estimated that, by 2030, the resulting air quality improvements would prevent 1400 premature deaths, almost 200,000 days of asthma symptoms, and 2.8 million days of acute respiratory problems, with cumulative health and environmental benefits of $7.5 billion (Government of Canada, 2015). Figure 10.4 provides an overview of potential health co-benefits and risks associated with a range of GHG mitigation sectors and measures.
Potential health co-benefits and risks of GHG mitigation measures.
Source
Adapted from Luehr, 2018.
Adaptation and GHG mitigation measures that do not consider human health implications can lead to negative health outcomes among the population, thus eroding climate resilience (Haines et al., 2009; Haines & Ebi, 2019). They may also lead to greater health inequities in the population, increasing the vulnerability of individuals and communities to future climate change (see Chapter 9: Climate Change and Health Equity). For example, a number of features of neighbourhoods can worsen health equity, including (PHAC, 2017):
lack of transportation options;
limited access to healthy food, housing, and health care;
lack of parks and recreation facilities;
empty buildings and vacant lots;
poor air or water quality;
lack of safety and higher crime;
increased social isolation; and
residential segregation.
Compared with GHG mitigation, there has been significantly less study of the potential health co-benefits and risks of climate change adaptation measures (Cheng & Berry, 2013). Health officials are recognizing the need for a systems-based approach to address climate change through GHG mitigation and adaptation; such an approach requires active and purposeful collaboration with other sectors, assessment of local vulnerabilities and capabilities, and the co-design of policies and programs based on this information (Ebi et al., 2016a; Ebi et al., 2016c). Efforts to achieve health co-benefits in the health sector by reducing GHGs and increasing climate resilience through adaptation offer a triple dividend for Canadians, specifically by (1) helping to make patients, staff, and communities safer during climate-related disasters and emergencies, (2) contributing to the slowing of climate change through the reduction of GHGs, and (3) achieving economic savings at health facilities that undertake adaptation efforts. The potential benefits are very large; in 2014, there were 798 hospitals across Canada with approximately 90,000 beds (CIHI, 2018). Health care facilities (particularly hospital campuses) have the highest intensity of energy use of all commercial and institutional buildings in Canada, and direct emissions increased between 2009 and 2015 at double the rate of the national average (Ribesse & Varangu, 2019). Figure 10.5 illustrates examples of features of low-carbon and resilient health care systems that overlap.
Climate-smart health care: the intersection of low-carbon health care and resilience.
Source
World Bank, 2017.
Globally, the average emissions per capita for health care activities is reported as 0.28 tonnes of carbon dioxide (tCO2) equivalent (Health Care Without Harm & ARUP, 2019). Canada’s health system has been identified as one of the top four emitters among countries, based on per capita emission of 1.1 tCO2 equivalent per capita (Health Care Without Harm & ARUP, 2019). The Canadian health sector as a whole, primarily hospitals, pharmaceuticals, and physician services, is estimated to have emitted between 4.6% and 5.1% (29.6–33 Mt CO2 equivalent) annually from 2009 to 2014, or 4.6% of total national GHG emissions in 2014 (Eckelman et al., 2018). Pichler et al. (2019) estimated the health carbon footprint of Organisation for Economic Co-operation and Development countries, which includes CO2 emissions related to providers of goods and services for health care, such as medical retailers, hospitals, ambulatory, long-term, or preventive health care. The health carbon footprint in Canada in 2014 was estimated to be 5.1% of the total national carbon footprint (Pichler et al., 2019). In 2017, at least 16 Canadian hospitals emitted more than 10 kt of GHGs (ECCC, 2019).
In Canada, 26% of health sector emissions arise directly from health care facilities and health care–owned vehicles and 13% indirectly from purchased energy sources, such as electricity, steam, cooling, and heating. The majority (61%) of GHGs from the health sector are attributed to the supply chain, which includes the production, transport, and disposal of goods and services, such as pharmaceuticals and other chemicals, food and agricultural products, medical devices, hospital equipment, and instruments (Health Care Without Harm, 2019). An estimated 68% of these carbon emissions are generated domestically, indicating that imported goods are also a significant contributor to these emissions.
Given the large amount of energy and supplies used by organizations in the health sector, such as hospitals, efforts to become more sustainable can result in huge economic and health dividends. The U.S. Environmental Protection Agency has estimated that health care facilities in the United States have saved more than 192 billion USD in energy costs over the last 20 years (Ribesse & Varangu, 2019). In another study, the Health Care Climate Council (2018) found that, if the U.S. health system reduced electricity use and carbon pollution by 30%, it would prevent 4130 premature deaths, 85,000 asthma attacks, 4 million respiratory symptom events, and 3750 hospital visits by 2030, resulting in savings of approximately 1.2 billion USD. Initiatives to improve energy conservation and reduce GHG emissions through adopting appropriate building design, purchasing energy efficient products, and incorporating renewable energy systems have potentially very large savings for Canadian hospitals; one study which is likely an underestimate suggested a savings of a cumulative $150 million per year in utility spending with an average payback period of seven years (Waddington & Varangu, 2016). Currently, Health Canada is working with the Standards Council of Canada to explore opportunities to integrate climate change information into building codes for hospitals.
Some hospitals in Canada are taking action to reduce their fossil fuel use and GHG emissions and therefore become more resilient (Waddington & Varangu, 2016). By reducing on-site energy use, hospitals can cope with longer periods of power outages using their limited standby power. One of the challenges in understanding GHG emissions reported from hospitals is the lack of consistency in how this information is tracked and reported. These inconsistencies make it difficult to consolidate information on progress in the health sector.
Canada can learn from actions taken by a number of international partners in efforts to reduce GHGs in the health sector and build climate resilience. Pichler et al. (2019) reported that 14 countries, mainly in Europe, have been able to reduce the health sector carbon footprint even while real expenditure continues to grow. The large potential to benefit human health and the environment is illustrated through the efforts taken by the U.K. National Health Service (NHS), which was the first health care system in the world to routinely report on GHG emissions. Similar to Canada, the NHS contributes between 4% and 5% of the country’s carbon footprint. The NHS has undertaken a concerted effort to understand where the GHGs are generated in the health system and has developed a carbon reduction strategy and a roadmap to reduce these emissions.
In 2016, the NHS Sustainable Development Unit for NHS England and Public Health England reported that the NHS reduced its carbon emissions by 11% between 2007 and 2015, exceeding the 10% target set in 2009 (National Health Service, 2016). The wider sector, which also includes public health and social care, saw a 13% reduction over the same period. These emission reductions occurred despite an 18% increase in health and social care activity. Carbon emissions reductions included a 16% reduction in relation to procurement, such as improvements to the footprint of pharmaceuticals; a 4% reduction in energy emissions through energy efficiency and conservation; and a 5% reduction in travel (National Health Service, 2016).
10.7
Knowledge Gaps
Share
New knowledge, partnerships, and capacity-building on climate change and health in the health sector in Canada have increased opportunities to use evidence-based information to make greater strides in efforts to protect Canadians from future impacts. Assessment tools and methods have been developed, for example, to examine the impacts of projected stresses and strains from climate change on health systems and facilities to gauge their resilience to climate change impacts. However, much research on climate change and health adaptation is not accessible and practical for decision making; few studies exist on the effectiveness of measures to protect health, the ease of implementation, and the capacity required for action (Banwell et al., 2018).
Previous national assessments and reports in Canada since 1995 have identified knowledge gaps that need to be filled to support decision makers’ efforts to prepare for climate change impacts on health (Royal Society of Canada, 1995; Health Canada, 1999; Health Canada, 2001; Health Canada, 2004; Séguin, 2008; Berry et al., 2014a; Brettle et al., 2016; Maguet, 2020). Disparities exist in the levels of research on climate change and health within each province and territory and across the country (Brettle et al., 2016). A review of Canadian research on climate change and health conducted from 2006 to 2016 found research on all of the identified gaps, but with wide variation in terms of the issue or region of Canada, focus, scale of research, and stage of knowledge maturation (e.g., limited numbers of field studies have been conducted and few interventions have been evaluated) (Kolnick, 2016). A much greater percentage of the 672 articles on climate change and health analyzed populations at increased risk, assessments, natural hazards, and food safety and/or security, compared to air quality, toxic substances, or psychosocial impacts. Only 11% of the articles focused on adaptation strategies and measures. In addition, the regional focus of research was also quite disparate, with many more articles examining climate change and health issues in Quebec, British Columbia, and Ontario, fewer in the North, and the least in other parts of Canada, particularly Nova Scotia, New Brunswick, and Prince Edward Island (Kolnick, 2016). A large proportion of the research addressed climate change and health from a national perspective. This may increase the relevance of these studies to a wider range of stakeholders but, in some cases, may decrease the capacity for these studies to inform local-level decision making and assessments.
The study likely did not capture research that incorporated Indigenous knowledge and so does not represent a complete picture of climate change and health research in Canada. However, significant knowledge gaps exist related to climate change and First Nations, Inuit, and Métis peoples’ health in Canada, including adaptation options (see Chapter 2: Climate Change and Indigenous Peoples’ Health in Canada). Many communities in Northern Canada have increased their capacity and expertise related to research management, research design, and interpretation and communication of study results (Abele & Gladstone, n.d.).
Further research is required in the following areas to support efforts to protect health and build climate-resilient health systems in Canada:
Adaptation measures
Identification of equitable, effective (including cost-effective) adaptation measures for reducing health risks from current climate variability and projected climate change.
Adaptation measures to address the health challenges and capacity issues First Nations, Inuit, and Métis peoples face from climate change, including rural, remote, and Northern communities.
Adaptation measures tailored for specific populations, for example, people experiencing homelessness (Kidd et al., 2020), children, and older populations and those living in rural, remote and Northern communities.
Adaptation measures to reduce risks to individuals and health systems from compounding and cascading events, including from possible non-linear changes in weather and future climate (Ebi et al., 2016a).
Technical and operational synergies among actions to reduce disaster risk and options to adapt to climate change and health (e.g., health facility emergency preparedness plans) (Banwell et al., 2018).
Novel, integrated, and multidisciplinary surveillance and monitoring for climate change and health (e.g., data collection and analysis, citizen science, laboratory diagnostics, meta-genomics, and geospatial mapping) (ECCC, 2020).
Standardized indicators of health risks posed by climate change, along with means of verification, similar to the indicators used to measure meteorological and climatological variables, to establish baselines for monitoring the effectiveness of adaptations (Cheng & Berry, 2013; Ebi et al., 2018a).
Identification of risk trade-offs associated with various health adaptations (e.g., can breathable fabric protect against bites by ticks and mosquitos?; ensuring green spaces that help cool health care facilities are designed to not attract disease-bearing vectors).
Identification of effective tools, dissemination methods, and approaches to communicate climate change and health to decision makers and the public (WHO, 2009).
Effective strategies for aligning climate change and health promotion efforts with communication activities to support the reduction of GHGs.
Information to support education efforts, communication of research findings, and resilience-building in First Nations, Inuit, and Métis communities, while supporting and strengthening the sharing and application of Indigenous knowledges including adaptation experiences.
Health system resilience
Current and projected climate-related impacts, vulnerabilities, and costs to health systems and facilities (e.g., health policies, programs, services, and infrastructure; health human resources planning, management, and training; and supply chains critical for health), including to rural, remote, and Northern health systems.
Current and projected climate-related impacts, vulnerabilities, and costs to health systems and facilities that serve First Nations, Inuit, and Métis
Effective adaptation and resilience-building measures for health systems and facilities, including rural, remote, and Northern health systems and those serving First Nations, Inuit, and Métis
Standardized GHG measurement methodologies (e.g., life-cycle assessment) for tracking health system and hospital GHG emissions to support targets and goals for the sector to reduce its carbon footprint and improve resilience.
Best approaches for reducing the carbon footprint of the health sector, for example, by retrofitting existing health care facilities.
Effective actions to address GHG emissions from the health sector supply chain, including evaluation of current purchasing practices in the Canadian health system and opportunities for suppliers to develop new, low-carbon products and services for the health sector.
Synergies between actions that support climate change resilience, adaptation, and environmental sustainability in the health system and those that support financial sustainability (i.e., savings from energy efficiency investments; telemedicine and virtual health care; electronic health care records; supply chain costs).
Easily accessible cooling technologies and practices that are not fossil-fuel-based for health care facilities, public cooling centres, and cooling for homes, both for new-builds and for retrofits of existing buildings.
Health co-benefits and risks of measures
Synergistic health co-benefits of various strategies to reduce GHG emissions to national targets that also reduce air pollution.
Direct and indirect health co-benefits and risks of measures taken by other sectors (e.g., water, agriculture, housing, transportation, insurance, energy, urban planning) to adapt to impacts (ECCC, 2020), including for First Nations, Inuit, and Métis peoples and rural, remote, and Northern communities.
Strategies that support health, including those that address the root causes of vulnerability and health inequities, and support the transition to a low-carbon economy in energy, agriculture, transportation, manufacturing, buildings, and other sectors.
Economic costs and benefits
Economic costs of the impacts of current climate variability and projected climate change on human health and health systems in Canada, as well as on social services that support the determinants of health.
Assessments of the economic costs and health co-benefits of GHG mitigation and adaptation activities (WHO, 2009; Huang et al., 2013).
Economic, social and health benefits of actions to build climate-resilient health systems (ECCC, 2020).
These research gaps cover a broad spectrum of climate change hazards and impacts on health as well as common public health and health system interventions to protect populations. Addressing these information needs would likely contribute to reducing threats to Canadians from other health risks such as pandemic disease, facilitating adaptation and resilience to a wide range of hazards.
10.8
Conclusion
Share
Climate change is a growing threat to the health of Canadians, communities, and health systems. Health systems and facilities in Canada are vulnerable to climate change, and many are already being affected by weather- and climate-related hazards. Climate change is increasing risks to health facility and health system staff, operations, and infrastructure. While many factors, such as future levels of inequity, social cohesion, and technological innovation will influence how the health of Canadians and their communities are affected by climate change, a major driver will be the resilience of health systems and the willingness and capacity of decision makers to take needed adaptive actions, in concert with partners in other sectors.
Adaptation actions to prepare Canadians, including those at higher risk, can be effective in reducing health impacts. For example, the recent response to the growing danger of extreme heat events through the development of HARS has reduced health risks and poor health outcomes in some countries. Robust adaptation to reduce health risks requires adaptation by a wide range of actors in society at multiple temporal and geographic scales that take into account complex drivers of poor health outcomes.
Analysis in this chapter suggests that a number of health authorities, from local to national levels, in Canada are taking adaptation actions to reduce health risks. However, fewer are taking concrete actions, such as developing a climate change and health program, dedicating targeted resources to adaptation, assessing resilience of critical health infrastructure, or training health professionals and staff. In addition, few provinces and territories have comprehensive (e.g., covering a wide range of likely risks to health) or substantive climate change and health adaptation actions as part of their broader climate change strategies, and no jurisdictions have a separate action plan or strategy that focuses exclusively on climate change and health. The wide diversity in efforts among health authorities, from local to national levels, with some taking aggressive action and others doing less, suggests many communities and health systems are at increased vulnerability to current and future projected impacts on health, including potentially very severe effects from compounding or cascading events.
10.8.1
Scaling Up Health Adaptation
Share
Rapidly scaling up health adaptation measures is needed to help protect Canadians from current health hazards and to reduce risks from climate change impacts in the future, such as extreme weather events that exceed adaptive thresholds. Health authorities should build upon past and current efforts to prepare for a warmer world, such as undertaking vulnerability and adaptation assessments for climate change and health, examining risks to health facilities from climate change, and implementing targeted adaptations such as early warning systems. This may require going outside of normal approaches used by ministries of health, such as expanding integrated monitoring and surveillance activities, mainstreaming information about climate risk into new programs and policies, as well as training clinicians, health researchers, and public health professionals about how to protect health in a changing climate.
10.8.2
Indigenous Leadership and Collaboration
Share
Progress in efforts to protect Canadians from climate change requires a commitment to upholding Indigenous leadership and partnership in research development and adaptation, including recognizing and using Indigenous knowledge in a respectful way. Inherent in these efforts is an openness to diverse ways of knowing and of learning from complementary and/or contrasting perspectives for adaptation decision-making. Respectful collaboration will ensure that actions to protect health are based on meaningful engagement informed by the unique circumstances and opportunities of Indigenous Peoples and Northern, remote, and rural communities, thereby respecting, upholding, and advancing the rights of Indigenous peoples.
10.8.3
Working with Other Sectors
Share
Adaptation progress will also require working more closely with decision makers outside of the health sector (e.g., water, agriculture, insurance, housing, energy, environment, emergency management, urban planning, transport, and infrastructure) to implement preventive and equitable measures to protect Canadians including by more vigorously addressing the social and environmental determinants of health. These activities should focus on opportunities to address barriers that limit preparedness (e.g., poverty, inadequate housing and infrastructure, ineffective communications), and to reduce uncertainty through increased collaborative research on impacts and effectiveness of adaptation.
Strong measures to reduce GHGs are needed to protect health and ensure that the ability of Canadians to adapt is not limited due to the severity of impacts. Very large health co-benefits can be achieved through multi-sectoral climate change adaptation to build resilience and through well-designed GHG mitigation efforts. Health decision makers have an important leadership role to play in raising awareness of these benefits and providing needed information to support robust efforts to address climate change through GHG mitigation (PHAC, 2017), including reducing the carbon footprint of the health sector, which is a major emitter of GHGs.
10.8.4
A National Health Adaptation Strategy
Share
National adaptation strategies for climate change and health must provide a comprehensive framework identifying key actors, accountabilities, priority areas of action, and clear goals and objectives. Such strategies can reduce future costs of preparedness through greater sharing of information and through more robust collaboration and coordination of efforts (WHO, 2021). The Government of Canada is developing its first ever national adaptation strategy that is expected to be released in 2023 (Government of Canada, 2021). A strong health component of a national strategy would include efforts to provide assistance to people and communities at highest risk through equitable adaptation measures. Actions would address the physical and operational risks of climate change to health systems and their infrastructure by supporting facility assessments, preparedness, and resilience-building, considering the special challenges faced by rural, remote and Indigenous health services and through efforts to update relevant codes and standards. It would enhance capacity for climate change and health modelling, forecasting, and state of the art early warning systems informed by surveillance of climate change and health indicators. A core component of a health adaptation strategy would be to work with other sectors to incorporate the perspectives, needs, and voices of equity-seeking groups and the general public. Considerations of social justice and integration of a gendered perspective into future climate change and health activities are needed to support resilience-building efforts; these considerations include empowering people disproportionately affected by climate change (e.g., Indigenous Peoples, women, people of low socio-economic status, immigrants) as educators, caregivers, holders of knowledge and agents of social change (Sorensen et al., 2018).
Greater efforts are needed to educate the public and decision makers about potential impacts and the benefits of preparedness to support scaled-up actions. This can include collaborating on climate change and health communications with the health care community and non-governmental organizations; increasing public health education using evidence-based advice and social marketing approaches; and developing a single window to provide easy access to climate change and health communication materials and messages (Brettle et al., 2016). Such activities would help Canadians, communities and their health systems move beyond responsive and more costly adaptation toward transformational adaptation that builds resilience to future climate change.
A national strategy could address many existing barriers to health adaptation, including limited social capital and ability to engage health relevant sectors, cognitive limits to behavioural change (Huang et al., 2011), a narrow framing of public health interventions that omits action on root causes of vulnerability (Gould & Rudolph, 2015) and the absence of coordinated planning among health sector partners at all levels of government. Through close collaboration, health decision makers, civil society partners, researchers, and members of the public can meet the challenge of climate change head-on, building more resilient health systems and communities to better protect health, now and in the future.
Footnotes
The term Indigenous is used in this chapter to refer collectively to the original inhabitants of Canada and their descendants, including First Nations, Inuit, and Métis peoples, as defined under Section 35 of the Constitution Act, 1982. Wherever possible, clear distinctions are made between these three distinct, constitutionally recognized groups. However, some generalizations are made, depending on the number and nature of citations used (e.g., Indigenous Peoples reflects more than one Indigenous group being referenced) and in instances where there may be shared experiences.
↩
Discussion of the contribution of Indigenous knowledge toward addressing climate change risks to health is found in Chapter 2: Climate Change and Indigenous Peoples’ Health in Canada.
↩
When possible indicators should be measurable or quantifiable, though in some cases qualitative information may be more meaningful to knowledge users. In all cases, indicators should reflect progress towards a meaningful objective. Example indicators may need to be adapted to reflect jurisdictional goals and realities.
↩
Yes = completed or substantially completed; Partially = actions underway but more effort needed; No = not completed or started.
↩
JF Consulting. (2020). Metis National Climate Change and Health Vulnerability Assessment. Not publicly available.
↩
Resilience indicators are shared with other categories.
↩
The health-in-all-policies approach requires decision makers in all sectors to integrate human health considerations and information into the development of policies and programs (PHAC, 2017).
↩
Anderson, H., Brown, C., Cameron, L. L., Christenson, M., Conlon, K. C., Dorevitch, S., Dumas, J., Eidson, M., Ferguson, A., Grossman, E., Hanson, A., Hess, J. J., Hoppe, B., Horton, J., Jagger, M., Krueger, S., Largo, T. W., Losurdo, G. M., Mack, S. R., Moran, C., … Walker, R. (2017). Climate and Health Intervention Assessment: Evidence on Public Health Interventions to Prevent the Negative Health Effects of Climate Change. Climate and Health Technical Report Series. Centers for Disease Control and Prevention. Retrieved from https://www.cdc.gov/climateandhealth/docs/ClimateAndHealthInterventionAssessment_508.pdf ↩
Arbuthnott, K., Hajat, S., & Heaviside, C. (2016). Changes in population susceptibility to heat and cold over time: assessing adaptation to climate change. Environmental Health, 15(S33). https://doi.org/10.1186/s12940-016-0102-7 ↩
Austin, S. E., Biesbroek, R., Berrang-Ford, L., Ford, J. D., Parker, S., & Fleury, M. D. (2016). Public Health Adaptation to Climate Change in OECD Countries. International Journal of Environmental Research and Public Health, 13(9), 889. https://doi.org/10.3390/ijerph13090889 ↩
Austin, S. E., Ford, J. D., Berrang-Ford, L., Biesbroek, R., & Ross, N. A. (2019). Enabling local public health adaptation to climate change. Social Science & Medicine (1982), 220, 236–244. https://doi.org/10.1016/j.socscimed.2018.11.002 ↩
Baccini, M., Kosatsky, T., Analitis, A., Anderson, H. R., D’Ovidio, M., Menne, B., … Biggeri, A. (2011). Impact of heat on mortality in 15 European cities: Attributable deaths under different weather scenarios. Journal of Epidemiology and Community Health, 65(1), 64–70. https://doi.org/10.1136/jech.2008.085639 ↩
Balbus, J., Berry, P., Brettle, M., Jagnarine-Azan, S., Soares, A., Ugarte, C., Varangu, L., & Prats, E. V. (2016). Enhancing the sustainability and climate resiliency of health care facilities: a comparison of initiatives and toolkits. Revista Panamericana de Salud Publica = Pan American Journal of Public Health, 40(3), 174–180.
↩
Banwell, N., Rutherford, S., Mackey, B., & Chu, C. (2018). Towards Improved Linkage of Disaster Risk Reduction and Climate Change Adaptation in Health: A Review. International Journal of Environmental Research and Public Health, 15(4), 793. https://doi.org/10.3390/ijerph15040793 ↩
Barreca, A., Clay, K., Deschenes, O., Greenstone, M., & Shapiro, J. S. (2016). Adapting to climate change: The remarkable decline in the US temperature-mortality relationship over the twentieth century. Journal of Political Economy, 124(1), 105-159.
↩
Beaudoin, M., & Gosselin, P. (2016). An effective public health program to reduce urban heat islands in Québec, Canada. Revista Panamericana de Salud Publica = Pan American Journal of Public Health, 40(3), 160–166.
↩
Benmarhnia, T., Bailey, Z., Kaiser, D., Auger, N., King, N., & Kaufman, J. S. (2016). A Difference-in-Differences Approach to Assess the Effect of a Heat Action Plan on Heat-Related Mortality, and Differences in Effectiveness According to Sex, Age, and Socioeconomic Status (Montreal, Quebec). Environmental Health Perspectives, 124(11), 1694–1699. https://doi.org/10.1289/EHP203 ↩
Benmarhnia, T., Zhao, X., Wang, J., Macdonald, M., & Chen, H. (2019). Evaluating the potential public health impacts of the Toronto cold weather program. Environment International, 127, 381–386. https://doi.org/10.1016/j.envint.2019.03.042 ↩
Berry, P., Clarke, K., Fleury, M. D., & Parker, S. (2014a). Human health. In F. J. Warren, & D. S. Lemmen (Eds.), Canada in a Changing Climate: Sector Perspectives on Impacts and Adaptation. Ottawa, ON: Government of Canada.
↩
Berry, P., Paterson, J., & Buse, C. (2014b). Assessment of vulnerability to the health impacts of climate change in Middlesex-London. Report prepared for the Middlesex-London Health Unit. London, United Kingdom. Retrieved from https://www.healthunit.com/climate-change ↩
Berry, P., Enright, P. M., Shumake-Guillemot, J., Villalobos Prats, E., & Campbell-Lendrum, D. (2018). Assessing Health Vulnerabilities and Adaptation to Climate Change: A Review of International Progress. International Journal of Environmental Research and Public Health, 15(12), 2626. https://doi.org/10.3390/ijerph15122626 ↩
Boeckmann, M., & Rohn, I. (2014). Is planned adaptation to heat reducing heat-related mortality and illness? A systematic review. BMC public health, 14, 1112. https://doi.org/10.1186/1471-2458-14-1112 ↩
Bouzid, M., Hooper, L., & Hunter, P. R. (2013). The effectiveness of public health interventions to reduce the health impact of climate change: a systematic review of systematic reviews. PloS One, 8(4), e62041. https://doi.org/10.1371/journal.pone.0062041 ↩
Brettle, M., MacMillan, K-A., Kolnick, L., & Berry, P. (2016). Climate change and health resiliency collaboration: Workshop report. Ottawa, ON: Health Canada.
↩
Bustinza, R., Lebel, G., Gosselin, P., Bélanger, D., & Chebana, F. (2013). Health impacts of the July 2010 heat wave in Québec, Canada. BMC Public Health, 13, 56. https://doi.org/10.1186/1471-2458-13-56 ↩
Campbell-Lendrum, D., Guillemot, J., & Ebi, K. L. (2015). Climate change and health vulnerability assessments: A Practical Approach. In G. Luber, & J. Lemery (Eds.), Global Climate Change and Human Health: From Science to Practice. San Francisco, CA: Jossey-Bass.
↩
Canadian Coalition for Green Health Care. (2018). Identifying methods, data sources and indicators of climate change impacts for assessing the resiliency of Canadian health care facilities. Report prepared for Health Canada.
↩
Casanueva, A., Burgstall, A., Kotlarski, S., Messeri, A., Morabito, M., Flouris, A. D., Nybo, L., Spirig, C., & Schwierz, C. (2019). Overview of Existing Heat-Health Warning Systems in Europe. International Journal of Environmental Research and Public Health, 16(15), 2657. https://doi.org/10.3390/ijerph16152657 ↩
Chau, P. H., Chan, K. C., & Woo, J. (2009). Hot weather warning might help to reduce elderly mortality in Hong Kong. International Journal of Biometeorology, 53(5), 461–468. https://doi.org/10.1007/s00484-009-0232-5 ↩
Cheng, J. J., & Berry, P. (2013). Health co-benefits and risks of public health adaptation strategies to climate change: a review of current literature. International journal of public health, 58(2), 305–311. https://doi.org/10.1007/s00038-012-0422-5 ↩
Ciscar, J. C., Feyen, L., Soria, A., Lavalle, C., Raes, F., Perry, M., Nemry, F., Demirel, H., Rozsai, M., Dosio, A., Donatelli, M., Srivastava, A., Fumagalli, D., Niemeyer, S., Shrestha, S., Ciaian, P., Himics, M., Van Doorslaer, B., Barrios, S., Ibáñez, N.,… Ibarreta, D. (2014). Climate Impacts in Europe. The JRC PESETA II Project. Luxembourg, Luxembourg: Publications Office of the European Union. Retrieved from https://publications.jrc.ec.europa.eu/repository/handle/JRC87011 ↩
Crump, J., Jacob, K., King, P., Mangalagiu, D., Zickgraf, C., Abiodun, B. J., Armiento, G., Bailey, R., Baker, E., Bowen, K. J., Dankelman, I., Djalante, R., Dutta, M., Hurley, F., Iraola, M. J., Kim, R. E., King, R., Kirilenko, A., dos Santos Lucon, O., Lyne, K., Martino, D., … Wright, C. Y. (2019). Systemic Policy Approaches for Cross-cutting Issues. In P. Ekins, J. Gupta, & P. Boileau (Eds.), Global Environment Outlook GEO-6: Healthy Planet, Healthy People (p. 425-448). Cambridge, United Kingdom: Cambridge University Press. Retrieved from https://wedocs.unep.org/handle/20.500.11822/27539 ↩
Curtis, S., Fair, A., Wistow, J., Val, D. V., & Oven, K. (2017). Impact of extreme weather events and climate change for health and social care systems. Environmental Health : A Global Access Science Source, 16(Suppl 1), 128. https://doi.org/10.1186/s12940-017-0324-3 ↩
Das, S., & Smith, S. C. (2012). Awareness as an adaptation strategy for reducing mortality from heat waves: evidence from a disaster risk management program in India, Climate Change Economics, 3(2), 1250010. https://doi.org/10.1142/S2010007812500108 ↩
de’ Donato, F. K., Leone, M., Scortichini, M., De Sario, M., Katsouyanni, K., Lanki, T., Basagaña, X., Ballester, F., Åström, C., Paldy, A., Pascal, M., Gasparrini, A., Menne, B., & Michelozzi, P. (2015). Changes in the Effect of Heat on Mortality in the Last 20 Years in Nine European Cities. Results from the PHASE Project. International Journal of Environmental Research and Public Health, 12(12), 15567–15583. https://doi.org/10.3390/ijerph121215006 ↩
Dodd, W., Scott, P., Howard, C., Scott, C., Rose, C., Cunsolo, A., & Orbinski, J. (2018). Lived experience of a record wildfire season in the Northwest Territories, Canada. Canadian journal of public health = Revue canadienne de sante publique, 109(3), 327–337. https://doi.org/10.17269/s41997-018-0070-5 ↩
Doyle, H., Malim, S., & Tapinder, F. S. (2017). Climate change and public health in Ontario. Ontario Public Health Association.
↩
Dupuis, J., & Biesbroek, R. (2013). Comparing apples and oranges: The dependent variable problem in comparing and evaluating climate change adaptation policies. Global Environmental Change, 23(6), 1476-1487. https://doi.org/10.1016/j.gloenvcha.2013.07.022 ↩
Ebi K. L. (2011a). Climate change and health risks: assessing and responding to them through ‘adaptive management’. Health affairs (Project Hope), 30(5), 924–930. https://doi.org/10.1377/hlthaff.2011.0071 ↩
Ebi K. L. (2011b). Resilience to the health risks of extreme weather events in a changing climate in the United States. International Journal of Environmental Research and Public Health, 8(12), 4582–4595. https://doi.org/10.3390/ijerph8124582 ↩
Ebi, K. L., & del Barrio, M. O. (2017). Lessons Learned on Health Adaptation to Climate Variability and Change: Experiences Across Low- and Middle-Income Countries. Environmental Health Perspectives, 125(6), 065001. https://doi.org/10.1289/EHP405 ↩
Ebi, K. L., Berry, P., Hayes, K., Boyer, C., Sellers, S., Enright, P. M., & Hess, J. J. (2018b). Stress Testing the Capacity of Health Systems to Manage Climate Change-Related Shocks and Stresses. International Journal of Environmental Research and Public Health, 15(11), 2370. https://doi.org/10.3390/ijerph15112370 ↩
Ebi, K. L., Boyer, C., Bowen, K. J., Frumkin, H., & Hess, J. (2018a). Monitoring and Evaluation Indicators for Climate Change-Related Health Impacts, Risks, Adaptation, and Resilience. International Journal of Environmental Research and Public Health, 15(9), 1943. https://doi.org/10.3390/ijerph15091943 ↩
Ebi, K. L., Boyer, C., Ogden, N., Paz, S., Berry, P., Campbell-Lendrum, D., Hess, J. J., & Woodward, A. (2021). Burning embers: synthesis of the health risks of climate change. Environmental Research Letters, 16(4), 044042. doi:10.1088/1748-9326/abeadd
↩
Ebi, K. L., Hess, J. J., & Isaksen, T. B. (2016c). Using Uncertain Climate and Development Information in Health Adaptation Planning. Current Environmental Health Reports, 3(1), 99–105. https://doi.org/10.1007/s40572-016-0077-0 ↩
Ebi, K. L., Hess, J. J., & Watkiss, P. (2017). Health risks and costs of climate change variability and change. In C. N. Mock, R. Nugent, O. Kobusingye, & K. R. Smith (Eds.), Injury prevention and environmental health: Disease control priorities (3rd, ed.). Washington, DC: World Bank Group.
↩
Ebi, K. L., & Semenza, J. C. (2008). Community-based adaptation to the health impacts of climate change. American Journal of Preventive Medicine, 35(5), 501–507. https://doi.org/10.1016/j.amepre.2008.08.018 ↩
Ebi, K. L., Semenza, J. C., & Rocklöv, J. (2016b). Current medical research funding and frameworks are insufficient to address the health risks of global environmental change. Environmental Health: A Global Access Science Source, 15(1), 108. https://doi.org/10.1186/s12940-016-0183-3 ↩
Ebi, K. L., Ziska, L. H., & Yohe, G. W. (2016a). The shape of impacts to come: Lessons and opportunities for adaptation from uneven increases in global and regional temperatures. Climatic Change, 139(3), 341-349. https://doi.org/10.1007/s10584-016-1816-9 ↩
Eckelman, M. J., Sherman, J. D., & MacNeill, A. J. (2018). Life cycle environmental emissions and health damages from the Canadian healthcare system: An economic-environmental-epidemiological analysis. PLoS Medicine, 15(7), e1002623. https://doi.org/10.1371/journal.pmed.1002623 ↩
Elliott, S. J., Bisung, E., Mulligan, K., & Wandel, J. (2017). Assessing Resilience of the Canadian Health System to the Impacts of Climate Change: A Proposed Analytical Framework. Report prepared for Health Canada. Ottawa, ON.
↩
Environics Research Group. (2017). Public Perceptions of Climate Change – Final Report. Report Prepared for Health Canada. Ottawa, ON.
↩
Eyzaguirre, J., & Warren, F. J. (2014). Adapting: Linking Research and Practice. In F. J. Warren, & D. S. Lemmen (Eds.), Canada in a Changing Climate: Sector Perspectives on Impacts and Adaptation (pp. 253–286). Ottawa, ON: Government of Canada.
↩
Ford, J. D., & King, D. (2015). A framework for examining adaptation readiness. Mitigation and Adaptation Strategies for Global Change, 20, 505-526. <https://doi.org/10.1007/s11027-013-9505-8>
↩
Ford, J. D., Sherman, M., Berrang-Ford, L., Llanos, A., Carcamo, C., Harper, S., Lwasa, S., Namanya, D., Marcello, T., Maillet, M., & Edge, V. (2018). Preparing for the health impacts of climate change in Indigenous communities: The role of communitybased adaptation. Global Environmental Change, 49, 129-139. <https://doi.org/10.1016/j.gloenvcha.2018.02.006>
↩
Fouillet, A., Rey, G., Wagner, V., Laaidi, K., Empereur-Bissonnet, P., Le Tertre, A., … Hémon, D. (2008). Has the impact of heatwaves on mortality changed in France since the European heatwave of summer 2003? A study of the 2006 heatwave. International Journal of Epidemiology, 37(2), 309–17. <https://doi.org/10.1093/ije/dym253>
↩
Friel, S. (2019). Climate Change and the People’s Health (N. Krieger, Ed). Oxford University Press.
↩
Friel, S., Bowen, K., Campbell-Lendrum, D., Frumkin, H., McMichael, A. J., & Rasanathan, K. (2011). Climate change, noncommunicable diseases, and development: the relationships and common policy opportunities. Annual Review of Public Health, 32, 133–147. https://doi.org/10.1146/annurev-publhealth-071910-140612 ↩
Frumkin, H., Hess, J., Luber, G., Malilay, J., & McGeehin, M. (2008). Climate change: the public health response. American Journal of Public Health, 98(3), 435–445. https://doi.org/10.2105/AJPH.2007.119362 ↩
Gosselin, P. (2010). Health of populations. In C. DesJarlais, M. Allard, D. Bélanger, A. Blondlot, A. Bouffard, A. Bourque, D. Chaumont, P. Gosselin, D. Houle, C. Larrivée, N. Lease, A. T. Pham, R. Roy, J.-P. Savard, R. Turcotte, & C. Villeneuve (Eds.), Learning to adapt to climate change. Montréal, QC: Ouranos. Retrieved from https://www.ouranos.ca/wp-content/uploads/RapportDesjarlais2010_EN.pdf ↩
Gosselin, P., Mehiriz, K., Tardif, I., Lemieux, M-A., & Beaudoin, S. (2018). Téléphone santé : un automate d’appel aux résultats prometteurs lors de vagues de chaleur ou de smog. Institut National de Santé Publique du Québec. Retrieved from
↩
Gould, S., & Rudolph, L. (2015). Challenges and Opportunities for Advancing Work on Climate Change and Public Health. International Journal of Environmental Research and Public Health, 12(12), 15649–15672. https://doi.org/10.3390/ijerph121215010 ↩
Government of Canada. (2020b). A healthy environment and a healthy economy: Canada’s strengthened climate plan to create jobs and support people, communities and the planet. Ottawa, ON. Retrieved from
↩
Green, S., Kim, S., Gaudet, M., & Cheung, E. (2018). Doctor’s prescription for cycling. Canadian family Physician Medecin de Famille Canadien, 64(10), 715–716.
↩
Hackett, F., Got, T., Kitching, G. T., MacQueen, K., & Cohen, A. (2020). Training Canadian doctors for the health challenges of climate change. The Lancet. Planetary health, 4(1), e2–e3. https://doi.org/10.1016/S2542-5196(19)30242-6 ↩
Haines, A., & Ebi, K. (2019). The Imperative for Climate Action to Protect Health. The New England Journal of Medicine, 380(3), 263–273. https://doi.org/10.1056/NEJMra1807873 ↩
Haines, A., McMichael, A. J., Smith, K. R., Roberts, I., Woodcock, J., Markandya, A., Armstrong, B. G., Campbell-Lendrum, D., Dangour, A. D., Davies, M., Bruce, N., Tonne, C., Barrett, M., & Wilkinson, P. (2009). Public health benefits of strategies to reduce greenhouse-gas emissions: overview and implications for policy makers. Lancet (London, England), 374(9707), 2104–2114. https://doi.org/10.1016/S0140-6736(09)61759-1 ↩
Hamilton, I., Kennard, H., McGushin, A., Höglund-Isaksson, L., Kiesewetter, G., Lott, M., Milner, J., Purohit, P., Rafaj., P., Sharma, R., Springman, M., Woodcock, J., & Watts, N. (2021). The public health implications of the Paris Agreement: a modelling study. Lancet Planetary Health, 5(2), e74-e83. https://doi.org/10.1016/S2542-5196(20)30249-7 ↩
Hathaway, J., & Maibach, E. W. (2018). Health Implications of Climate Change: a Review of the Literature About the Perception of the Public and Health Professionals. Current Environmental Health Reports, 5(1), 197–204. https://doi.org/10.1007/s40572-018-0190-3 ↩
Health Canada. (1999). CAPITALizing on Science: Report of a Workshop on Climate Change, Science and Health. Canadian Journal of Public Health. ↩
Health Canada. (2001). How will climate change affect priorities for your health science and policy research? [Conference]. First annual national health and climate change science and policy research consensus conference. Ottawa, ON.
↩
Health Canada. (2004). Climate change and health: Research report. Ottawa, ON.
↩
Hess, J. J., & Ebi, K. L. (2016). Iterative management of heat early warning systems in a changing climate. Annals of the New York Academy of Sciences, 1382(1), 21–30.
↩
Hess, J., Lm, S., Knowlton, K., Saha, S., Dutta, P., Ganguly, P., Tiwari, A., Jaiswal, A., Sheffield, P., Sarkar, J., Bhan, S., Begda, A., Shah, T.A., Solanki, B., & Mavalankar, D. (2018). Building Resilience to Climate Change: Pilot Evaluation of the Impact of India’s First Heat Action Plan on All-Cause Mortality. Journal of Environmental and Public Health, 2018(9). https://doi.org/10.1155/2018/7973519 ↩
Heudorf, U., & Schade, M. (2014). Heatwaves and mortality in Frankfurt am Main, Germany, 2003-2013: what effect do heat-health action plans and the heat warning system have? Zeitschrift fur Gerontologie und Geriatrie, 47(6), 475–482. <https://doi.org/10.1007/s00391-014-0673-2>
↩
Hill, J. (2012). Analysis of Climate Change and Health-Promotion Campaigns in Relation to Heat-Health Messages. Report prepared for Health Canada. Ottawa, ON.
↩
Hoegh-Guldberg, O., Jacob, D., Taylor, M., Bindi, M., Brown, S., Camilloni, I., Dieghiou, A., Djalante, R., Ebi, K. L., Engelbrecht, F., Guiot, J., Hijioka, Y., Mehrotra, S., Payne, A., Seneviratne, S. I., Thomas, A., Warren, R., & Zhou, G. (2018). Impacts of 1.5ºC Global Warming on Natural and Human Systems. In V. Masson-Delmotte, P. Zhai, H.-O. Pörtner, D. Roberts, J. Skea, P. R. Shukla, A. Pirani, W. Moufouma-Okia, C. Péan, R. Pidcock, S. Connors, J. B. R. Matthews, Y. Chen, X. Zhou, M.I.Gomis, E. Lonnoy, T.Maycock, M.Tignor, & T. Waterfield (Eds.), Global Warming of 1.5°C. An IPCC Special Report on the impacts of global warming of 1.5°C above pre-industrial levels and related global greenhouse gas emission pathways, in the context of strengthening the global response to the threat of climate change, sustainable development, and efforts to eradicate poverty. Cambridge, United Kingdom: Cambridge University Press.
↩
Hondula, D. M., Balling, R. C., Vanos, J. K., & Georgescu, M. (2015). Rising Temperatures, Human Health, and the Role of Adaptation. Current Climate Change Reports, 1(3), 144–154. https://doi.org/10.1007/s40641-015-0016-4 ↩
Huang, C., Vaneckova, P., Wang, X., Fitzgerald, G., Guo, Y., & Tong, S. (2011). Constraints and barriers to public health adaptation to climate change: a review of the literature. American Journal of Preventive Medicine, 40(2), 183–190. https://doi.org/10.1016/j.amepre.2010.10.025 ↩
Huang, C., Barnett, A. G., Xu, Z., Chu, C., Wang, X., Turner, L. R., & Tong, S. (2013). Managing the health effects of temperature in response to climate change: challenges ahead. Environmental Health Perspectives, 121(4), 415–419. https://doi.org/10.1289/ehp.1206025 ↩
Hunt, A., Ferguson, J., Baccini, M., Watkiss, P., & Kendrovski, V. (2017) Climate and weather service provision: Economic appraisal of adaptation to health impacts. Climate Services, 7, 78–86. https://doi.org/10.1016/j.cliser.2016.10.004 ↩
Hutton, G., & Menne, B. (2014). Economic evidence on the health impacts of climate change in Europe. Environmental Health Insights, 8, 43–52. <https://doi.org/10.4137/EHI.S16486>
↩
Interior Health. (2017). @Interior Health: A publication for staff and physicians of IH.
↩
Intergovernmental Panel on Climate Change (IPCC). (2014). Climate change 2014: Synthesis Report. Contribution of Working Groups I, II and III to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change (Core Writing Team, R. K. Pachauri & L. A. Meyer, Eds.). Geneva, Switzerland.
↩
Janssen I. (2012). Health care costs of physical inactivity in Canadian adults. Applied Physiology, Nutrition, and Metabolism = Physiologie Appliquee, Nutrition et Metabolisme, 37(4), 803–806. <https://doi.org/10.1139/h2012-061>
↩
Jarrett, J., Woodcock, J., Griffiths, U. K., Chalabi, Z., Edwards, P., Roberts, I., & Haines, A. (2012). Effect of increasing active travel in urban England and Wales on costs to the National Health Service. Lancet (London, England), 379(9832), 2198–2205. https://doi.org/10.1016/S0140-6736(12)60766-1 ↩
Jay, O., Capon, A., Berry, P., Broderick, C., de Dear, R., Havenith, G., Honda, Y., Kovats, R.S., Ma, W., Malik, A., Morris, N.B., Nybo, L., Seneviratne, S.I., Vanos, J., Ebi, K.L. Heat and Health 2 – Reducing the health effects of hot weather and heat extremes: from personal cooling strategies to green cities. The Lancet. Vol 398: 709–24. https://pubmed.ncbi.nlm.nih.gov/34419206/ ↩
Kennedy, E., Olsen, H., Vanos, J., Vecellio, D. J., Desat, M., Richters, K., Rutledge, A., & Richardson, G. (2021). Reimagining spaces where children play: developing guidance for thermally comfortable playgrounds in Canada. Canadian Journal of Public Health = Revue Canadienne de Sante Publique, 112(4), 706–713. https://doi.org/10.17269/s41997-021-00522-7 ↩
Kidd, S. A., Greco, S. & McKenzie, K. (2020). Global Climate Implications for Homelessness: A Scoping Review. Journal of Urban Health, 98, 385-393. https://doi.org/10.1007/s11524-020-00483-1 ↩
King, N., Bishop-Williams, K. E., Beauchamp, S., Ford, J. D., Berrang-Ford, L., Cunsolo, A., IHACC Research Team., & Harper, S. L. (2019). How do Canadian media report climate change impacts on health? A newspaper review. Climatic Change, 152, 581-596. https://doi.org/10.1007/s10584-018-2311-2 ↩
Knowledge Management. (2018). Towards a Pan-Canadian surveillance system for climate-related health
indicators: Final report. Kingston, ON: KFL&A Public Health.
↩
Kolnick, L. (2016). Analysis of a decade of climate change and health research in Canada: Are researchers making progress in addressing identified knowledge gaps?. Report prepared for Health Canada.
↩
Kovats, S., Lloyd, S., Hunt, A., & Watkiss, P. (2011). The Impacts and Economic Costs on Health in Europe and the Costs and Benefits of Adaptation. Technical Policy Briefing Note Series. Oxford, United Kingdom: Stockholm Environment Institute.
↩
KPMG. (2017). May 2016 Wood Buffalo Wildfire Post-Incident Assessment Report. Report prepared for Alberta Emergency Management Agency. Prepared for Alberta Emergency Management Agency. Retrieved from https://www.alberta.ca/assets/documents/Wildfire-KPMG-Report.pdf ↩
Kuchmij, N., Berry, P., Enright, P., Schnitter, R., & Hamilton, S. (2020). Climate and Health Vulnerability & Adaptation Assessments: A Knowledge to Action Resource Guide. Ottawa, ON: Health Canada.
↩
Kyselý, J., & Plavcová, E. (2012). Declining impacts of hot spells on mortality in the Czech Republic, 1986–2009: Adaptation to climate change? Climatic Change, 113, 437–453.
↩
L’Hérault, E., Michel, A., Fortier, D., Carbonneau, A-S., Doyon-Robitaille, J., Lachance, M-P., Ducharme, M-A., Larrivée, K., Grandmont, K., & Lemieux, C. (2013). Production de cartes prédictives des caractéristiques du pergélisol afin de guider le développement de l’environnement bâti pour les communautés du Nunavik. Rapport final. Québec, QC : Centre d’études nordiques, Université Laval.
↩
Lesnikowski, A., Ford, J., Berrang-Ford, L., Paterson, J., Barrera, M., & Heymann, S. (2011). Adapting to health impacts of climate change: A study of UNFCCC Annex I parties. Environmental Research Letters, 6(4), 044009. doi:10.1088/1748-9326/6/4/04400
↩
Levison, M. M., Butler, A. J., Rebellato, S., Armstrong, B., Whelan, M., & Gardner, C. (2018). Development of a Climate Change Vulnerability Assessment Using a Public Health Lens to Determine Local Health Vulnerabilities: An Ontario Health Unit Experience. International Journal of Environmental Research and Public Health, 15(10), 2237. https://doi.org/10.3390/ijerph15102237 ↩
Limaye, V. S., Max., W., Consitible., J., & Knowlton, K. (2019). Estimating the health-related costs of 10 climate-sensitive U.S. events during 2012. GeoHealth, 3(9), 245-265. https://doi.org/10.1029/2019GH000202 ↩
Luehr, G. (2018). Health co- ‘benefits’ and ‘risks’ in climate change mitigation technologies and policies: A review for Canada. Report Prepared for Health Canada.
↩
MacIntyre, E., Khanna, S., Darychuk, A., Copes, R., & Schwartz, B. (2019). Evidence synthesis – Evaluating risk communication during extreme weather and climate change: a scoping review. Health Promotion and Chronic Disease Prevention in Canada : Research, Policy and Practice, 39(4), 142–156. https://doi.org/10.24095/hpcdp.39.4.06 ↩
Maibach, E. (2019). Increasing public awareness and facilitating behavior change: Two guiding heuristics. In L. Hannah & T. Lovejoy (Eds.), Climate Change and Biodiversity (2nd ed.) Yale University Press.
↩
Man, R. X., Lack, D. A., Wyatt, C. E., & Murray, V. (2018). The effect of natural disasters on cancer care: a systematic review. The Lancet. Oncology, 19(9), e482–e499. https://doi.org/10.1016/S1470-2045(18)30412-1 ↩
Martinez, G. S., Berry, P., Balbus, J., Hodgson, T., Salazar, M. Sellers, S., & Hess, J. (2018). The adaptation health gap: A global overview. In H. Neufeldt, G. S. Martinez, A. Olhoff, C. Knudsen, & K. Dorkenoo (Eds.), The Adaptation Gap Health Report. Nairobi, Kenya: United Nations Environment Programme (UNEP). Retrieved from https://www.unep.org/resources/adaptation-gap-report-2018 ↩
Martinez, G. S., Linares, C., Ayuso, A., Kendrovski, V., Boeckmann, M., & Diaz, J. (2019). Heat-health action plans in Europe: Challenges ahead and how to tackle them. Environmental Research, 176, 108548. https://doi.org/10.1016/j.envres.2019.108548 ↩
Mehiriz, K., & Gosselin, P. (2019). Evaluation of the Impacts of a Phone Warning and Advising System for Individuals Vulnerable to Smog. Evidence from a Randomized Controlled Trial Study in Canada. International Journal of Environmental Research and Public Health, 16(10), 1817. https://doi.org/10.3390/ijerph16101817 ↩
Mehiriz, K., Gosselin, P., Tardif, I., & Lemieux, M. A. (2018). The Effect of an Automated Phone Warning and Health Advisory System on Adaptation to High Heat Episodes and Health Services Use in Vulnerable Groups-Evidence from a Randomized Controlled Study. International Journal of Environmental Research and Public Health, 15(8), 1581. https://doi.org/10.3390/ijerph15081581 ↩
Michelozzi, P., De Sario, M., Accetta, G., de’Donato, F., Kirchmayer, U., D’Ovidio, M., Perucci, C. A., & HHWWS Collaborative Group (2006). Temperature and summer mortality: geographical and temporal variations in four Italian cities. Journal of Epidemiology and Community Health, 60(5), 417–423. https://doi.org/10.1136/jech.2005.040857 ↩
Miller, F., Bytautas, J.P., & Feng, P. (2018). Opportunities for engaging Canadian health systems in addressing the challenge of climate change. Retrieved from https://ssrn.com/abstract=3167088 ↩
Missirian, A., & Schlenker, W. (2017). Asylum applications respond to temperature fluctuations. Science (New York, N.Y.), 358(6370), 1610–1614. https://doi.org/10.1126/science.aao0432 ↩
Morabito, M., Profili, F., Crisci, A., Francesconi, P., Gensini, G. F., & Orlandini, S. (2012). Heat-related mortality in the Florentine area (Italy) before and after the exceptional 2003 heat wave in Europe: an improved public health response?. International journal of biometeorology, 56(5), 801–810. https://doi.org/10.1007/s00484-011-0481-y ↩
National Academies of Sciences, Engineering, and Medicine (NASEM). (2018). Protecting the health and well-being of communities in a changing climate: Proceedings of a workshop. Washington, DC: The National Academies Press.
↩
Noble, I. R., Huq, S., Anokhin, Y. A., Carmin, J., Goudou, D., Lansigan, F. P., Osman-Elasha, B., & Villamizar, A. (2014). Adaptation needs and options. In C. B. Field, , V. R. Barros, D. J. Dokken, K. J. Mach, M. D. Mastrandrea, T. E. Bilir, M. Chatterjee, K. L. Ebi, Y. O. Estrada, R. C. Genova, B. Girma, E. S. Kissel, A. N. Levy, S. MacCracken, P. R. Mastrandrea, & L. L. White (Eds.), Climate Change 2014: Impacts, Adaptation, and Vulnerability. Part A: Global and Sectoral Aspects. Contribution of Working Group II to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change. Cambridge, United Kingdom and New York, NY, USA: Cambridge University Press.
↩
Paavola, J. (2017). Health impacts of climate change and health and social inequalities in the UK. Environmental Health, 16, 113. https://doi.org/10.1186/s12940-017-0328-z ↩
Paterson, J. A., Ford, J. D., Berrang-Ford, L., Lesnikowski, A., Berry, P., Henderson, J., & Heymann, J. (2012). Adaptation to climate change in the Ontario public health sector. BMC Public Health, 12, 452. https://doi.org/10.1186/1471-2458-12-452 ↩
Paterson, J., Berry, P., Ebi, K., & Varangu, L. (2014). Health care facilities resilient to climate change impacts. International Journal of Environmental Research and Public Health, 11(12), 13097–13116. https://doi.org/10.3390/ijerph111213097 ↩
Pichler, P. P., Jaccard, I. S., Weisz, U., & Weisz, H. (2019). International comparison of health care carbon
footprints Environmental Research Letters, 14(6), 064004. https://doi.org/10.1016/S2542-5196(20)30121-2 ↩
Roles, A. (2013). Southern Alberta Flood. Presented to the Canadian Healthcare Network.
↩
Royal Society of Canada. (1995). Implications of global change for human health: Final report of the health issues panel of the Canadian Global Change Program. Incidental Report. No IR95-2.
↩
Schifano, P., Leone, M., De Sario, M., de’Donato, F., Bargagli, A. M., D’Ippoliti, D., Marino, C., & Michelozzi, P. (2012). Changes in the effects of heat on mortality among the elderly from 1998-2010: results from a multicenter time series study in Italy. Environmental Health : A Global Access Science Source, 11, 58. https://doi.org/10.1186/1476-069X-11-58 ↩
Scott, D., Minano, A., Chakraborty, L., Henstra, D., Thistlethwaite, J., & Apajee, Y. (2020). Flood risk analysis of Canadian health and emergency infrastructure. Climate Risk Research Group, University of Ottawa.
↩
Sellers, S., & Ebi, K. L. (2017). Climate change and health under the shared socioeconomic pathway framework. International Journal of Environmental Research and Public Health, 15(1), 3. https://doi.org/10.3390/ijerph15010003 ↩
Shapiro, L. T., Gater, D. R., Jr, Espinel, Z., Kossin, J. P., Galea, S., & Shultz, J. M. (2020). Preparing individuals with spinal cord injury for extreme storms in the era of climate change. EClinicalMedicine, 18, 100232. https://doi.org/10.1016/j.eclinm.2019.12.002 ↩
Sheridan, S. C., & Allen, M. J. (2018). Temporal trends in human vulnerability to excessive heat. Environmental Research Letters, 13(4), 043001. https://doi.org/10.1088/1748-9326/aab214 ↩
Sheridan, S. C., & Dixon, P. G. (2016). Spatiotemporal trends in human vulnerability and adaptation to heat across the United States. Anthropocene, 20, 61-73. https://doi.org/10.1016/j.ancene.2016.10.001 ↩
Shin, Y. S., & Ha, J. (2012). Policy Directions Addressing the Public Health Impact of Climate Change in South Korea: The Climate-change Health Adaptation and Mitigation Program. Environmental Health and Toxicology, 27, e2012018. https://doi.org/10.5620/eht.2012.27.e2012018 ↩
Shindell, D.T., Lee, Y., & Faluveg, G. (2016). Climate and health impacts of US emissions reductions consistent with 2oC. Nature Climate Change, 6(5), 503-507. doi:10.1038/nclimate2935, 2016.
↩
Shindell, D. T., Faluvegi, G., Seltzer, K., & Shindell C. (2018). Quantified, localized health benefits of accelerated carbon dioxide emission reductions. Nature Climate Change, 8(4), 291-295. doi:10.1038/s41558-018-0108-y
↩
Shumake-Guillemot, J., Amir, S., Anwar, N., Arrighi, J., Böse-O’Reilly, S., Brearley, M., Cross, J., Daanen, H., … Zaitchik, B. (2020). Technical brief: Protecting health from hot weather during the COVID-19 pandemic. Global Heat Health Information Network. Retrieved from http://www.ghhin.org/assets/technical-brief-COVID-and-Heat-final.pdf ↩
Smith, K. R., Woodward, A., Campbell-Lendrum, D., Chadee, D. D., Honda, Y., Liu, Q., . . . Sauerborn, R. (2014). Human health: Impacts, adaptation, and co-benefits. In C. B. Field, V. R. Barros, D. J. Dokken, K. J. Mach, M. D. Mastrandrea, T. E. Bilir, M. Chatterjee, K. L. Ebi, Y. O. Estrada, R. C. Genova, B. Girma, E. S. Kissel, A. N. Levy, S. MacCracken, P. R. Mastrandrea, & L. L. White (Eds.), Climate change 2014: Impacts, adaptation, and vulnerability. Part A: Global and sectoral aspects. Contribution of Working Group II to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change (pp. 709-754). Cambridge, United Kingdom: Cambridge University Press. Retrieved from https://www.ipcc.ch/report/ar5/wg2/ ↩
Springmann, M., Godfray, H. C., Rayner, M., & Scarborough, P. (2016). Analysis and valuation of the health and climate change cobenefits of dietary change. Proceedings of the National Academy of Sciences of the United States of America, 113(15), 4146–4151. https://doi.org/10.1073/pnas.1523119113 ↩
Survey Research Centre. (2019). Survey of health sector officials: A contribution to Health Canada’s Climate Change and Health Adaptation Capacity Building Program and the National Assessment – Technical and data analysis report. Report prepared for Health Canada. University of Waterloo.
↩
Tan, J., Zheng, Y., Song, G., Kalkstein, L. S., Kalkstein, A. J., & Tang, X. (2007). Heat wave impacts on mortality in Shanghai, 1998 and 2003. International Journal of Biometeorology, 51(3), 193–200. https://doi.org/10.1007/s00484-006-0058-3 ↩
Valois, P., Jacob, J., Mehiriz, K., Talbot, D., Renaud, J.-S., & Caron, M. (2018). Portrait de l’adaptation aux changements climatiques dans les organisations du secteur de la santé au Québec. Québec, QC: Université Laval.
↩
Valois, P., Talbot, D., Caron, M., Carrier, M.-P., Morin, A. J. S., Renaud, J.-S., Jacob, J. & Gosselin, P. (2017). Development and Validation of a Behavioural Index for Adaptation to High Summer Temperatures among Urban Dwellers. International Journal of Environmental Research and Public Health, 14(7), 820. https://doi.org/10.3390/ijerph14070820 ↩
Vodden, K., & Cunsolo, A. (2021). Rural and Remote Communities. In F. J. Warren & N. Lulham (Eds.), Canada in a Changing Climate: National Issues Report. Ottawa, ON: Government of Canada. Retrieved from https://changingclimate.ca/national-issues/ ↩
Waddington, K., & Varangu, L. (2016). Canadian Coalition for Green Health Care Leading the Evolution of Green. Healthcare Quarterly (Toronto, Ont.), 19(3), 23–29. https://doi.org/10.12927/hcq.2016.24869 ↩
Waddington, K., Varangu, L., Berry, P., & Paterson, J. (2013). Preparing for the health impacts of climate change: How ready is your health care organization? Journal of the Canadian Healthcare Engineering Society, 1, 34–39.
↩
Wardekker, J. A., de Jong, A., van Bree, L., Turkenburg, W. C., & van der Sluijs, J. P. (2012). Health Risks of Climate Change: An Assessment of Uncertainties and Its Implications for Adaptation Policies. Environmental Health, 11(67). https://doi.org/10.1186/1476-069X-11-67 ↩
Watts, N., Adger, W. N., Agnolucci, P., Blackstock, J., Byass, P., Cai, W., Chaytor, S., Colbourn, T., Collins, M., Cooper, A., Cox, P. M., Depledge, J., Drummond, P., Ekins, P., Galaz, V., Grace, D., Graham, H., Grubb, M., Haines, A., Hamilton, I., … Costello, A. (2015). Health and climate change: policy responses to protect public health. Lancet (London, England), 386(10006), 1861–1914. https://doi.org/10.1016/S0140-6736(15)60854-6 ↩
Watts, N., Amann, M., Arnell, N., Ayeb-Karlsson, S., Beagley, J., Belesova, K., Boykoff, M., Byass, P., Cai, W., Campbell-Lendrum, D., Capstick, S., Chambers, J., Coleman, S., Dalin, C., Daly, M., Dasandi, N., Dasgupta, S., Davies, M., Di Napoli, C., Dominguez-Salas, P., … Costello, A. (2021). The 2020 report of The Lancet Countdown on health and climate change: responding to converging crises. Lancet (London, England), 397(10269), 129–170. https://doi.org/10.1016/S0140-6736(20)32290-X ↩
Watts, N., Amann, M., Ayeb-Karlsson, S., Belesova, K., Bouley, T., Boykoff, M., Byass, P., Cai, W., Campbell-Lendrum, D., Chambers, J., Cox, P. M., Daly, M., Dasandi, N., Davies, M., Depledge, M., Depoux, A., Dominguez-Salas, P., Drummond, P., Ekins, P., Flahault, A., … Costello, A. (2018). The Lancet Countdown on health and climate change: from 25 years of inaction to a global transformation for public health. Lancet (London, England), 391(10120), 581–630. https://doi.org/10.1016/S0140-6736(17)32464-9 ↩
Weinberger, K. R., Zanobetti, A., Schwartz, J., & Wellenius, G. A. (2018). Effectiveness of National Weather Service heat alerts in preventing mortality in 20 US cities. Environment international, 116, 30–38. https://doi.org/10.1016/j.envint.2018.03.028 ↩
Weisskopf, M. G., Anderson, H. A., Foldy, S., Hanrahan, L. P., Blair, K., Török, T. J., & Rumm, P. D. (2002). Heat wave morbidity and mortality, Milwaukee, Wis, 1999 vs 1995: an improved response?. American Journal of Public Health, 92(5), 830–833. https://doi.org/10.2105/ajph.92.5.830 ↩
Wondmagegn, B. Y., Xiang, J., Williams, S., Pisaniello, D., & Bi, P. (2019). What do we know about the healthcare costs of extreme heat exposure? A comprehensive literature review. The Science of the Total Environment, 657, 608–618. https://doi.org/10.1016/j.scitotenv.2018.11.479 ↩
Woodcock, J., Abbas, A., Ullrich, A., Tainio, M., Lovelace, R., Sá, T. H., Westgate, K., & Goodman, A. (2018). Development of the Impacts of Cycling Tool (ICT): A modelling study and web tool for evaluating health and environmental impacts of cycling uptake. PLoS Medicine, 15(7), e1002622. https://doi.org/10.1371/journal.pmed.1002622 ↩
World Health Organization (WHO). (2013). Protecting Health from Climate Change: Vulnerability and Adaptation Assessment. Retrieved from http://www.who.int/iris/handle/10665/104200 ↩
World Health Organization (WHO). (2018a). WHO UNFCCC Climate Health Country Profile Project—Monitoring Health Impacts of Climate Change and Progress in Building Climate Resilient Health Systems.
↩
World Health Organization (WHO). (2020). WHO guidance for climate-resilient and environmentally sustainable health care facilities. Geneva, Switzerland. Retrieved from https://www.who.int/publications/i/item/9789240012226 ↩
Zhang, X., Flato, G., Kirchmeier-Young, M., Vincent, L., Wan, H., Wang, X., Rong, R., Fyfe, J., Li, G., & Kharin, V. V. (2019). Changes in temperature and precipitation across Canada. In E. Bush & D.S. Lemmen (Eds.), Canada’s Changing Climate Report. Ottawa, ON: Government of Canada. Retrieved from <https://changingclimate.ca/CCCR2019>
↩